


Mortality trends due to concomitant cardiovascular disease and cancer in the United States
 0
0 Abstract
Aim: Cancer and cardiovascular disease (CVD), although often perceived as distinct entities, are complexly interrelated and share numerous common risk factors. Despite increasing attention to deaths from cancer and CVD, studies on mortality trends due to concomitant CVD and cancer remain limited. Therefore, this study sought to assess trends in mortality with both cancer and CVD listed as causes of death in the United States across key demographic and state-level subgroups.
Methods: The data used in this study was obtained from the Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research dataset and the US Census Bureau. The analysis included deaths occurring from 2000 to 2023 among persons aged 15 years or older with both cancer and CVD listed as causes of death.
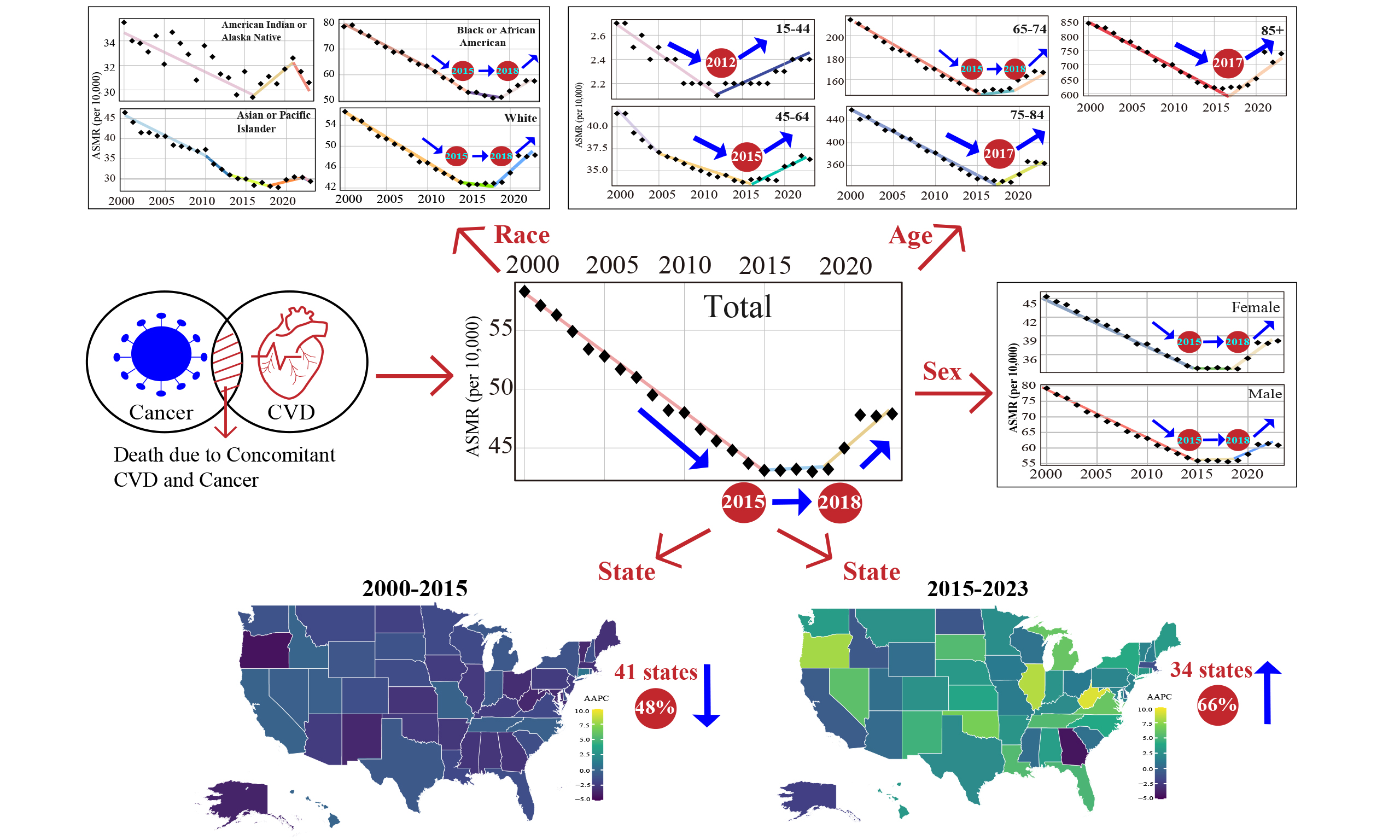
Results: From 2000 to 2015, age-adjusted mortality rate due to concomitant cancer and CVD decreased significantly, then declined at a slower and non-significant rate until 2018. After 2018, interestingly, a significant upward trend emerged. This pattern of falling first and then rising was consistent across most demographic subgroups, except for American Indian or Alaska Native and Asian or Pacific Islander population. Notably, the timing of the upward inflection point varied across subgroups, with the youngest individuals (aged 15-44 years) being the first to transition to an upward trend. Geographically, from 2000 to 2015, significant decreases occurred in 41 states (80%). In contrast, from 2015 to 2023, a significant increase was observed in 34 states(66%). Proportion analysis indicates that the observed increase in mortality due to concomitant cancer and CVD represents a true increase in the burden of death due to concomitant cancer and CVD rather than an artifact stemming solely from independent changes in mortality for each individual disease.
Conclusion: These findings underscore the critical need for enhanced intervention strategies targeting mortality risk associated with comorbid due to concomitant cancer and CVD.
Keywords
INTRODUCTION
Currently, there is increasing attention on the mortality due to concomitant cancer and cardiovascular disease (CVD), because these two disease types often share common risk factors, including aging, inflammation, oxidative stress, metabolic abnormalities, immune dysregulation, and so on[1]. In addition, although rapid advancements in cancer detection and treatment have prolonged patient survival, the cardiotoxic effects of anti-tumor therapy have also increased the risks of CVD and cardiovascular mortality among cancer survivors[2]. On the other hand, the incidence of cancer has also been reported to be higher in patients with cardiovascular disease compared to the general population[3]. Moreover, medications used to treat cardiovascular disease may promote cancer development[4,5]. The above emphasizes the importance of research on the prevention and management of death due to concomitant cancer and CVD.
Therefore, in recent years, the study of cardiac oncology has been widely of interest and has made rapid progress. However, there are still few studies on the mortality trends due to concomitant cancer and CVD at the national level, and most epidemiological studies focus on the mortality risk of a single disease, rather than the intersection of the two.
Considering the aging of the population and the constant changes in the treatment of cancer and CVD, it is urgent to understand the changes in the death burden due to concomitant cancer and CVD. Therefore, the purpose of this study was to evaluate the mortality trends due to concomitant cancer and CVD in the United States (U.S.) from 2000 to 2023. Analyses were stratified by age, sex, race, and geographic region to identify high-risk subgroups and evolving disease patterns, with the goal of informing targeted interventions to improve outcomes in this population.
METHODS
Study design
The data used in this study was obtained from the Centers for Disease Control and Prevention (CDC) Wide-ranging Online Data for Epidemiologic Research (WONDER) dataset dataset and the US Census Bureau. Data were extracted from the CDC WONDER dataset, which provides regularly updated death certificate information for U.S. residents coded according to the International Classification of Diseases, Tenth Revision (ICD-10)[6,7]. We downloaded cause-specific death counts from the Current Final Multiple Cause of Death Data 1999-2020 and the Provisional Multiple Cause of Death Data 2018-Last Week.
Data collection
We sourced the mortality data between 2000 and 2023 from the Multiple Cause-of-Death database of CDC WONDER. We utilized the Multiple Cause-of-Death Public Use Files to identify deaths for which both an ICD-10 code for cancer (C00-C97) and an ICD-10 code for cardiovascular disease (I00-I78) were listed among the multiple causes of death[7,8]. Only mortality in individuals 15 years and older was included in the present analysis. Mortality trends were stratified based on age, gender, race, and state. Race was categorized as American Indian or Alaska Native, Asian or Pacific Islander, Black or African American, and White-consistent with classifications used in prior CDC WONDER analyses[8]. Age groups were categorized into five groups: 15-44 years, 45-64 years, 65-74 years, 75-84 and 85 above. Considering that the death burden of the elderly population is more obvious, the age division of the elderly population is more detailed. Similar stratifications have been used in prior research as well[9,10].
Statistical analysis
Age-adjusted mortality rates (ASMRs) per 100,000 population with 95% confidence intervals (CIs) were calculated by standardizing death counts using annual U.S. Census population totals and the 2000 U.S. standard population[11]. ASMR trend of patients with comorbid cancer and CVD was assessed using annual percent change (APC) and average annual percent change (AAPC) with 95% CIs[12]. The APC and AAPC were considered statistically significant if the slope describing the mortality trend over each time interval was significantly different from zero, as assessed by a two-tailed t-test. Statistical significance was predefined at a threshold of P < 0.05[12]. Joinpoint regression identified inflection points, with analyses stratified by gender, age, race, and state. To examine the influence of covariates on temporal trend inflection points, we included interaction terms between time and each covariate in the Bayesian hierarchical model. Subgroup analyses were performed to evaluate trends stratified by sex, race, age group, and U.S. state, in order to explore variations across demographic and geographic dimensions. To address potential false discovery due to the large number of stratified analyses, a multiple comparison correction was applied. Details of Bayesian hierarchical model and multiple comparison correction are provided in the Supplementary Materials. The U.S. state-level map was generated in R version 4.3.3 using the ggplot2, sf and rnaturalearth packages, based on administrative boundary data from the openly accessible Natural Earth dataset. All other statistical analyses and graphing were performed using R version 4.3.3 (R Foundation) and Joinpoint Regression version 4.9.1.0 (National Cancer Institute).
RESULTS
Over the entire period from 2000 to 2023, we found that the overall trend in ASMR due to concomitant cancer and CVD showed a decline in the total population (AAPC 2000-2023: -0.7823, P < 0.05), as well as in both females (AAPC 2000-2023: -0.6739, P < 0.05) and males (AAPC 2000-2023: -1.1174, P < 0.05) [Supplementary Table 1]. But specifically, the ASMR due to concomitant cancer and CVD in the total population significantly decreased before 2015. However, this declining trend reversed after 2015. The ASMR plateaued, remaining stable until 2018, and then increased significantly to 2023 [Figure 1A]. To verify the robustness of the inflection points identified in 2015 and 2018, we conducted a confirmatory analysis using hierarchical Bayesian models adjusted for state-level covariates, including drug-related mortality, opioid overdose mortality, and PM2.5 concentration. The results indicated that the inflection points in 2015 and 2018 remained robust and were not confounded by these covariates [Supplementary Table 2]. Subsequently, a sensitivity analysis employing the 2010 US standard population was performed, which demonstrated that the timing of these inflection points (2015 and 2018) remained unchanged, thereby arguing against a potential cohort effect [Supplementary Figure 1].
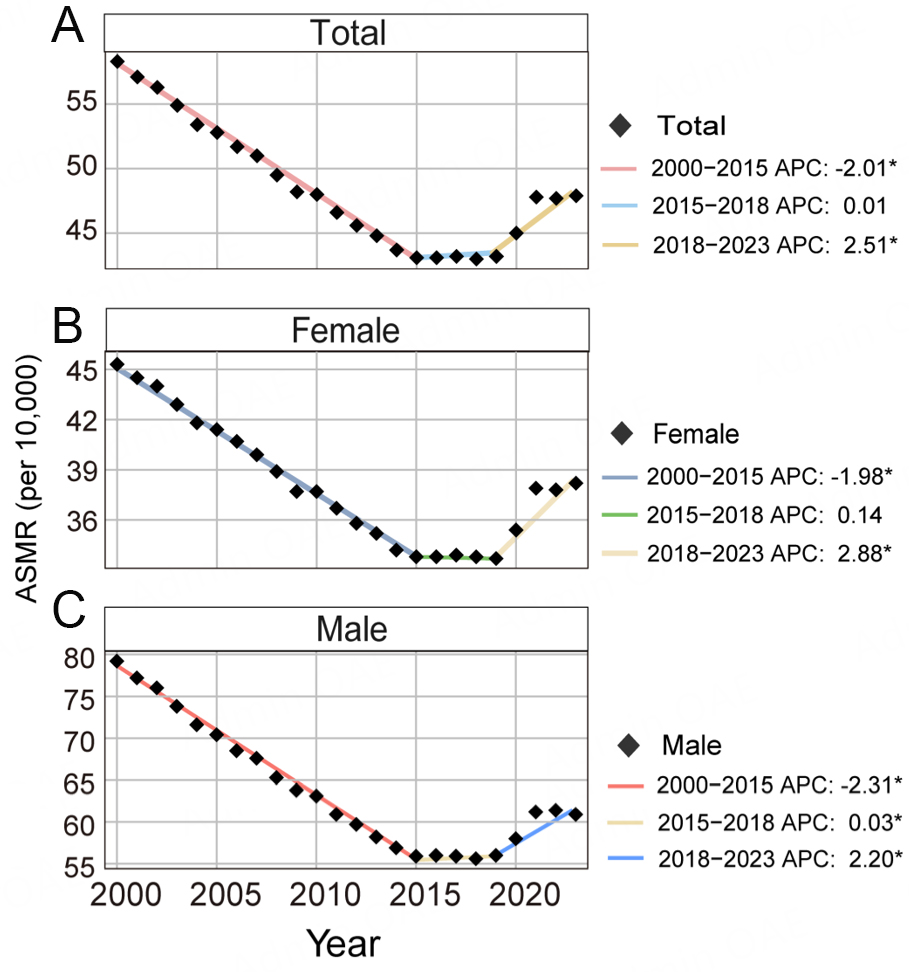
Figure 1. Trends of the ASMR attributable to comorbid cancer and cardiovascular disease among (A) total, (B) female and (C) male in the United States from 2000 to 2023. *P < 0.05, ASMR: Age-standardized mortality rates; APC: annual percent change.
In sex-stratified analyses, inflection points similar to those in the overall population were observed. The ASMR due to concomitant cancer and CVD in females also exhibited an initial significant decline from 2000 to 2015 , followed by a plateau until 2018, and then a significant rise to 2023 [Figure 1B]. In contrast, the trend of the ASMR due to concomitant cancer and CVD in males comprised a significant decline from 2000 to 2015, a gentle increase until 2018, and then a significant rise to 2023 [Figure 1C]. Total population, males and females shared the same inflection points in the trend of ASMR due to concomitant cancer and CVD, in 2015 and 2018 [Figure 1A-C].
Furthermore, from 2000 to 2023, the proportion of ASMR due to concomitant cancer and CVD within both the cancer ASMR (AAPC 2000-2023: 0.6339, P < 0.05) and the cardiovascular disease ASMR (AAPC 2000-2023: 1.2132, P < 0.05) showed a significant overall increasing trend, with an inflection point observed in 2015 for both [Supplementary Table 3; Figure 2A and B]. Notably, the proportion within the cancer ASMR decreased significantly before 2015 and increased significantly thereafter [Figure 2A]. In contrast, the trend of proportion of ASMR due to concomitant cancer and CVD within the overall ASMR showed no significant net change (AAPC 2000-2023: -0.0365, P > 0.05) over the entire 2000-2023 period
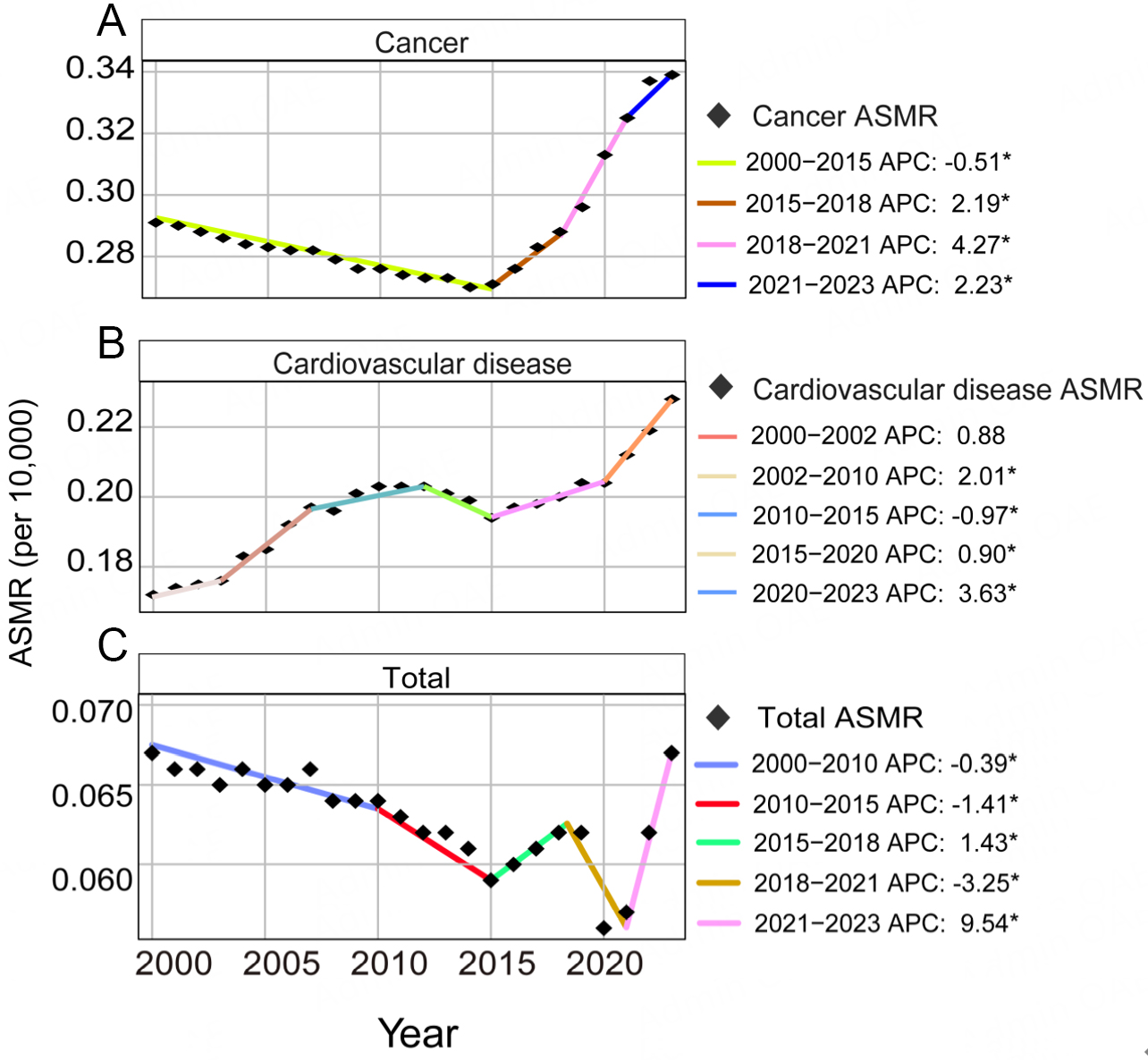
Figure 2. Trends in the proportion of the ASMR attributable to comorbid cancer and cardiovascular diseases within (A) the cancer ASMR, (B) the cardiovascular ASMR , and(C) the overall ASMR in the United States from 2000 to 2023. *P < 0.05, ASMR: Age-standardized mortality rates; APC: annual percent change.
From 2000 to 2023, broadly, the overall trend in ASMR due to concomitant cancer and CVD exhibited a consistent pattern across all age groups: an initial decline followed by a subsequent increase [Figure 3]. Specifically, the trends in ASMR due to concomitant cancer and CVD across different age groups were as follows: in the 15-44 years group, a significant decrease was observed before 2012, followed by a significant increase thereafter [Figure 3A]; in the 45-64 years group, a significant decline occurred before 2016, turning to a significant rise after 2016 [Figure 3B]; for the 65-74 years group, a significant decrease was noted before 2015, remained stable until 2018, and then shifted to a significant upward trend [Figure 3C]; in both the 75-84 years and the 85 above years groups, a significant decline was seen before 2017, shifting to a significant increase after 2017 [Figure 3D and E].
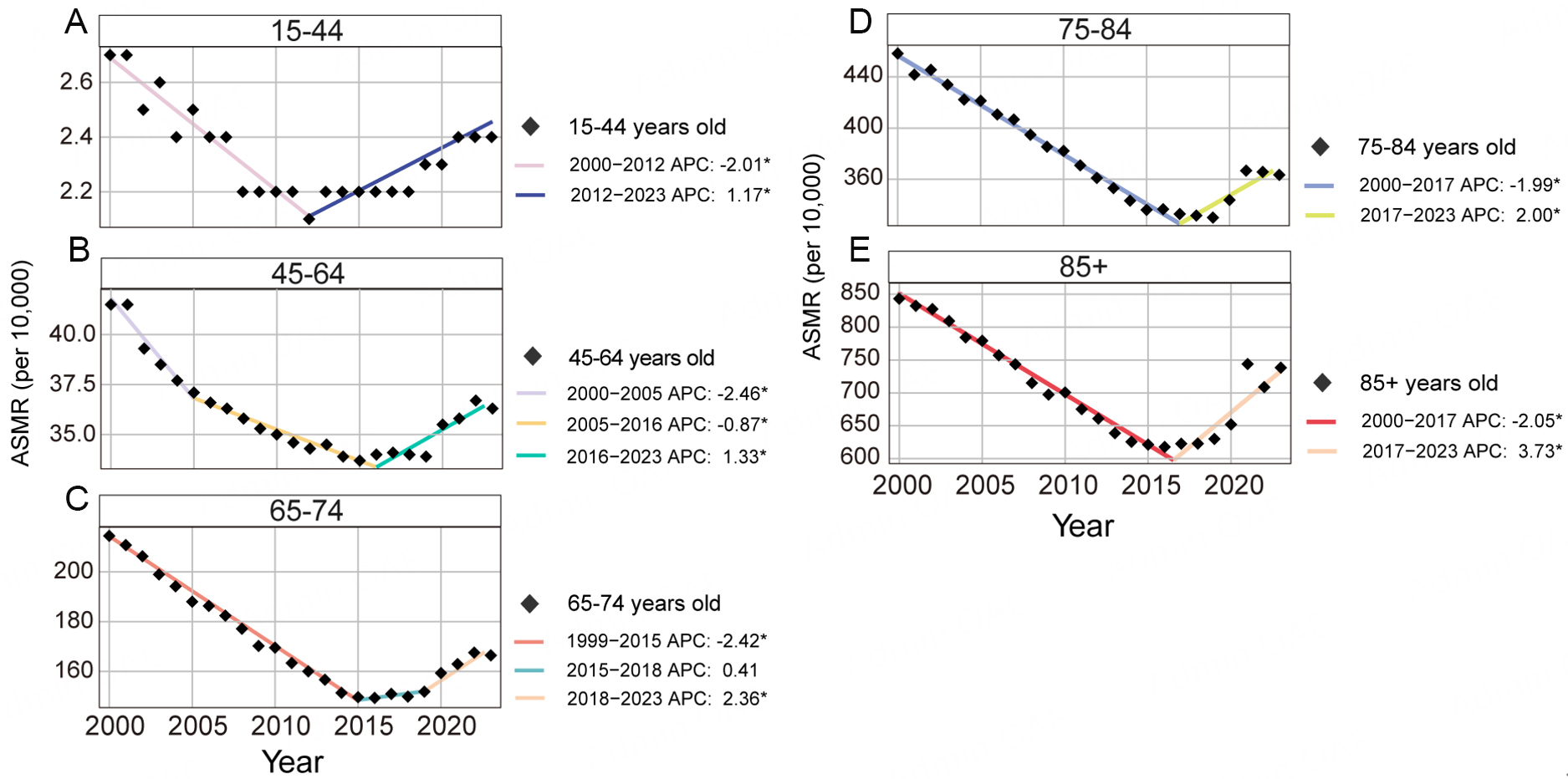
Figure 3. Trends of the ASMR attributable to comorbid cancer and cardiovascular disease among (A) 15-44 years old, (B) 45-64 years old, (C) 65-74 years old, (D) 75-84 years and (E) 85+ years old in the United States from 2000 to 2023. *P < 0.05, ASMR: Age-standardized mortality rates; APC: annual percent change.
Regarding racial disparities, the American Indian or Alaska Native population exhibited a significant decrease in ASMR due to concomitant cancer and CVD from 2000 to 2016, followed by a non-significant increase from 2016 to 2021, and then a non-significant decline from 2021 to 2023 [Figure 4A]. For the Asian or Pacific Islander population, the ASMR trend showed a significant decrease from 2000 to 2018, a significant increase from 2018 to 2021, and finally a non-significant decline from 2021 to 2023 [Figure 4B]. As for Black or African American and White populations, ASMR due to concomitant cancer and CVD all exhibited a significant increase after 2018. Prior to 2018, however, distinct patterns were observed in ASMR due to concomitant cancer and CVD in Black or African American and White populations: the Black or African American group showed a significant decrease from 2000 to 2015, followed by a stable period with no significant change from 2015 to 2018; while the White group demonstrated a consistent significant decline throughout the period before 2018 [Figure 4C and D].
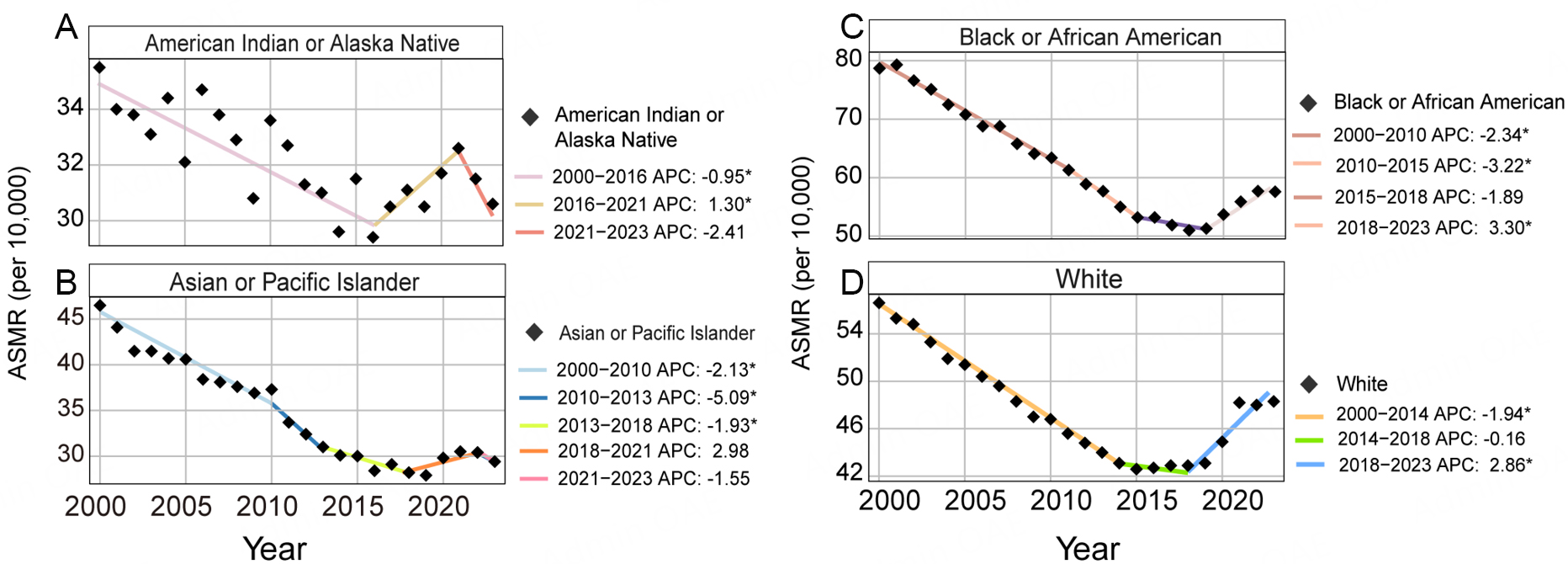
Figure 4. Trends of ASMR attributable to comorbid cancer and cardiovascular disease among (A) American Indian or Alaska Native, (B) Asian or Pacific Islander, (C) Black or African American, and (D) White in the United States. *P < 0.05, ASMR: Age-standardized mortality rates; APC: annual percent change.
This study incorporated state-level data from the US. Based on the reversal the downward trend of ASMR due to concomitant cancer and CVD in the total population observed in 2015 in the US, this year was therefore selected as the temporal cutoff for state-level comparisons. In most states, the analysis revealed that the AAPC of ASMR due to concomitant cancer and CVD exhibited a significant declining trend before 2015, which reversed to a significant increase thereafter [Supplementary Table 4; Figure 5]. Specifically, from 2000 to 2015, a significant decline (AAPC < 0, P < 0.05) in ASMR due to concomitant cancer and CVD was observed in 41 states (80%). During the same period, no significant change (P > 0.05) in CVD-related ASMR among cancer patients was observed in 9 states (18%) and significant increases (AAPC > 0, P < 0.05) were found only in Connecticut [Supplementary Table 4; Figure 5A]. In contrast, from 2015 to 2023, a significant increase (AAPC > 0, P < 0.05) in CVD-related ASMR among cancer patients was observed in 34 states (66%). During the same period, 13 states (25%) showed no significant change (P > 0.05), while significant declines (AAPC < 0; P < 0.05) were observed in Alaska, Georgia, Idaho and North Dakota [Supplementary Table 4; Figure 5B]. It is noteworthy that the statistical significance of both the overall mortality trend measured by the AAPC and the major inflection points determined by the APC remained unchanged across demographic and geographic subgroups after correction for multiple comparisons.
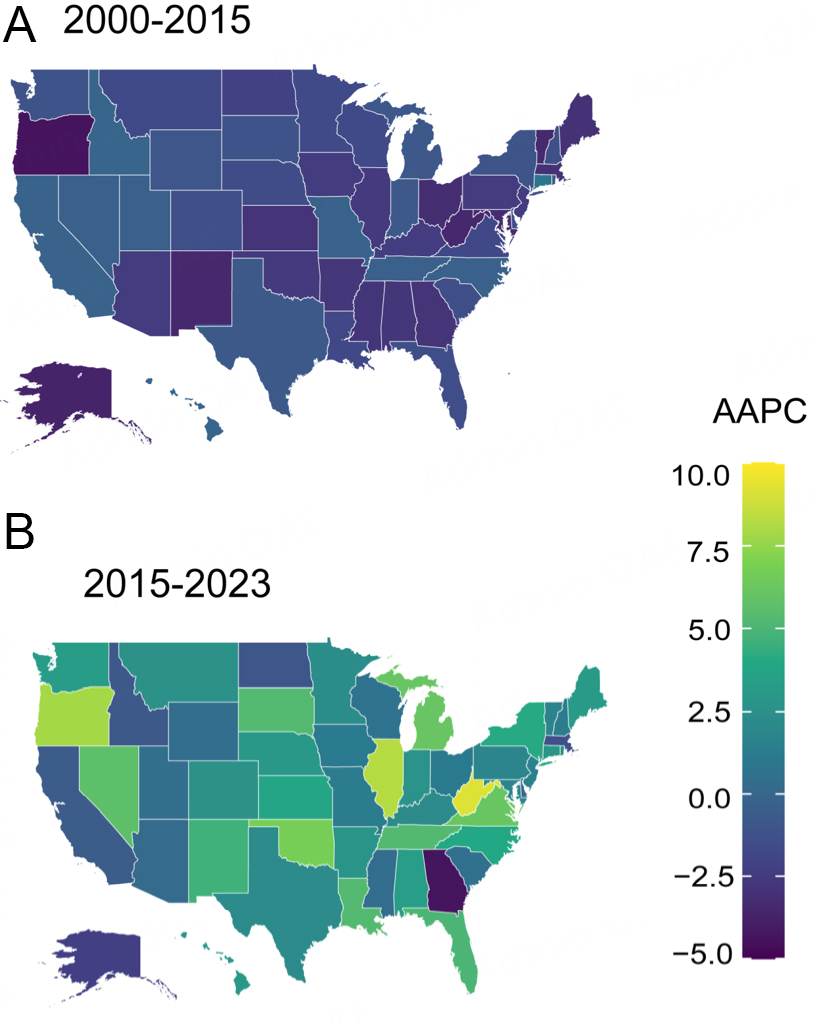
Figure 5. Geographic trends in the ASMR due to comorbid cancer and cardiovascular disease in the United States for the periods (A) 2000-2015 and (B) 2015-2023. *P < 0.05, ASMR: Age-standardized mortality rates; AAPC: average annual percentage change.
DISCUSSION
This nationwide study delineates the trend in death burden due to concomitant cancer and CVD in the United States from 2000 to 2023. The ASMR for this comorbidity showed an overall pattern of decline until 2015, stabilized through 2018, and then increased significantly thereafter. Furthermore, a hierarchical Bayesian model confirmed that the inflection points around 2015 and 2018 were robust and not confounded by geographic or socio-environmental factors. Subsequently, a sensitivity analysis using the 2010 U.S. standard population yielded consistent results, arguing against a cohort effect. This convergent evidence strongly supports the reliability of the identified temporal patterns.
The reversal of the long-term downward trend in ASMR after 2015, evolving into a period of relative stability and then a significant increase post-2018, is a central and concerning finding. The initial decline observed before 2015 was likely driven by advances from the preceding decades, including improvements in cancer screening, the efficacy of traditional therapies, and robust primary and secondary prevention of CVD (e.g., management of hypertension and dyslipidemia). Enhanced monitoring for treatment-related cardiotoxicity may have also played a role.
The plateau and subsequent rise in the trend after 2015 may be attributed to multiple factors. First, the dramatic expansion of the cancer survivor population, with its extended survival, provides the necessary timeframe for long-term, cumulative cardiovascular toxicities to manifest. These cardiovascular toxicities arise from cumulative damage caused by both traditional treatment regimens (e.g., anthracyclines, radiotherapy) and novel therapeutic agents[3,13]. Specifically, while transformative for cancer survival, newer drug classes like immune checkpoint inhibitors and certain kinase inhibitors are associated with distinct cardiovascular toxicities whose clinical presentation can be delayed[14]. Thus, therapeutic success paradoxically enlarges the at-risk cohort for these iatrogenic complications. Secondly, the death risk caused by cancer and CVD is compounded by two concurrent population-level trends: a rising burden of shared metabolic disorders (obesity, metabolic syndrome, diabetes) that provide a common pathological substrate accelerating both diseases, and increasing exposure to adverse lifestyle and environmental risk factors[15]. Furthermore, the formalization of cardio-oncology as a subspecialty since the mid-2010s has improved the clinical recognition and accurate attribution of deaths to this comorbidity[16], which may have contributed to the observed rise in reported ASMR. The COVID-19 pandemic, beginning in late 2019, likely exacerbated the post-2018 trajectory by disrupting routine care[17].
Supplementary analysis of the proportion of ASMR due to concomitant cancer and CVD within all-cause, cancer-specific, and CVD-specific ASMR provided important context. The concurrent "decline-then-rise" pattern in the proportion of ASMR due to concomitant cancer and CVD within both cancer-specific and CVD-specific ASMR robustly indicates that the increase in ASMR reflects a true rise in the burden of this comorbidity, not merely an artifact of changing mortality rates for each disease in isolation. In contrast, the proportion of ASMR due to concomitant cancer and CVD within all-cause ASMR showed a significant transient decline from 2018 to 2021. This decline is most plausibly explained by the massive, acute increase in all-cause ASMR due to COVID-19 pandemic during this period[18], which mechanically reduced the proportional contribution of nearly all other causes of ASMR. The post-2021 rebound, therefore, likely represents a statistical re-equilibration as the acute pandemic mortality shock subsided, rather than a sudden biological change in the death risk due to concomitant cancer and CVD. Equally important, this decline pattern argues against the possibility that the overall observed trends are merely an artifact of improved surveillance or diagnostic coding over time. If the trend in mortality were solely due to increasing detection (surveillance bias), we would not expect to see such a clear, temporally aligned reversal with the COVID-19 pandemic, coinciding with an exogenous shock of this magnitude. The fact that the data captures this expected perturbation supports the robustness and validity of our primary time-series analysis.
Furthermore, our stratified analysis of mortality trends across different populations revealed that all age groups exhibited a similar overarching "decline-then-rise" pattern, although some groups experienced a period of stability during the transition. The specific timing of the inflection points, however, varied by age group. Notably, the trend reversal occurred earliest in the youngest cohort (15-44 years), around 2012. This may be because younger patients with cancer and CVD may have a higher prevalence of underlying genetic predispositions, which elevates the incidence and mortality of both conditions[3,19]. Additionally, young adults with cancer are more likely to receive high-intensity, curative-intent therapies, whose cardiovascular toxicity has a latency period of years to a decade. The benefits of treatment advances from the early 2000s, combined with the earlier adoption of novel agents with cardiotoxic potential (e.g., kinase inhibitors, immune checkpoint inhibitors) in this group, meant that the cumulative burden of these long-term cardiovascular toxicities began converting into observable increases in mortality after 2012[14]. Concurrently, shared metabolic risk factors like obesity and diabetes have risen earlier and more sharply in younger generations, potentially amplifying treatment-related toxicity and disease progression[20,21]. Finally, their longer post-treatment life expectancy provides a wider time window for long-term cardiovascular toxicity to emerge. Together, these elements explain why the mortality trend for this group reversed several years before the national average. These findings underscore the critical need to prioritize cardio-oncology surveillance and primary prevention strategies specifically for adolescents and young adults. For example, health promotion activities aimed at young people should be promoted more widely to reduce the common risk factors (such as obesity, lack of exercise and smoking) that lead to cancer and CVD death.
Regarding racial disparities, Black or African American and White populations exhibited trends similar to the overall pattern. In contrast, the American Indian or Alaska Native population showed a rise only from 2016 to 2021, and the Asian or Pacific Islander population trend showed an initial decline followed by stability through 2023, without transitioning to a significant increase. This indicates that future prevention and public health strategies for cancer and CVD comorbidity may need to be prioritized for Black or African American and White populations. But it is also crucial, this focus on the largest at-risk groups does not preclude the need for parallel, culturally specific strategies for other racial and ethnic groups, whose distinct risk profiles, as shown in this analysis, demand equally tailored research and intervention.
State-level analysis revealed that trends in most states were consistent with the overall national pattern, with a shift around 2015 from a significant decline to either an increase or a stabilized trend. Heterogeneity across states exists, and this geographic variation may reflect differences in healthcare infrastructure, demographic composition, implementation of cardio-oncology monitoring programs, and regional disparities in risk factor prevalence or cancer treatment patterns. This necessitates future state-specific, targeted public health strategies for preventing and managing death due to concomitant cancer and CVD.
Strengths and weaknesses
This study has several strengths, including the use of a large, nationally representative dataset spanning 23 years, which allows for robust trend analysis and subgroup stratification. The application of joinpoint regression provides an objective method to identify significant inflection points in mortality trends. Furthermore, this study has revealed a potential population-level signal of rising mortality due to concomitant cancer and CVD in recent years, providing a critical foundation for subsequent clinical and public policy research.
However, several limitations must be acknowledged. Firstly, our reliance on death certificate data is subject to inherent limitations, including the risks of coding errors, misclassification, and incomplete information. More specifically, the observed temporal trends could have been artifactually influenced by secular changes in clinical awareness, diagnostic intensity, and death certificate coding practices. For instance, the formalization of cardio-oncology, the adoption of more sensitive diagnostic tools, and revisions to coding guidelines, particularly if their implementation accelerated around inflection points such as 2015 and 2018, could systematically increase the likelihood that both cancer and cardiovascular disease are identified and recorded as contributing causes of death over time. This may lead to an artificial increase in recorded mortality attributable to concomitant CVD and cancer, independent of a true change in population disease burden. Secondly, the lack of detailed data on cancer types, specific cardiovascular diagnoses, and detailed treatment history (including specific agents, cumulative doses, and treatment sequencing) limits our ability to establish direct mechanistic links. Third, the absence of key clinical variables, such as smoking history, body mass index, hypertension, diabetes, and socioeconomic status, prevents risk adjustment and the exploration of potential confounding factors. Finally, racial categories are social constructs and may not capture biological diversity; observed differences are more likely rooted in systemic inequities, which our data cannot fully elucidate.
In conclusion, the increasing mortality due to concomitant cancer and CVD in recent years has underscored the pressing need for the proactive management of underlying conditions and risk factors common to both cancer and CVD. Especially in the era of continuously evolving cancer therapies, it is crucial to advance the development of cardio-oncology service systems, establish evidence-based monitoring guidelines, and address age-related, geographic and racial disparities in access to diagnosis and treatment.
DECLARATIONS
Authors’ contributions
Writing – review & editing, writing – original draft, investigation, formal analysis, data curation, conceptualization: Cai J
Writing – review & editing, writing – original draft, supervision, investigation, conceptualization: Zhou B
Availability of data and materials
CDC Wonder data was publicly available at https://wonder.cdc.gov/. Analysis data was available from corresponding author.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This study has been funded by the National Natural Science Foundation of China (32470826), Tsinghua University (ZY01_07) and the Beijing Municipal Health Commission (2024-3-034).
Conflicts of interest
Zhou B is a Youth Editorial Board Member of The Journal of Cardiovascular Aging. Zhou B was not involved in any steps of the editorial processing, notably including reviewer selection, manuscript handling, or decision-making. Cai J declared that there are no conflicts of interest.
Ethical approval and consent to participate
This study was based on publicly available, de-identified data obtained from the CDC WONDER database and the U.S. Census Bureau. Therefore, ethical approval and informed consent were not required.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Alhuneafat L, Guha A, Blaes A, Konety SH. Cancer and cardiovascular disease: shared risk factors, mechanisms, and clinical implications: JACC: cardiooncology state-of-the-art review. JACC CardioOncol. 2025;7:453-69.
2. Cleary S, Rosen SD, Gilbert DC, Langley RE. Cardiovascular health: an important component of cancer survivorship. BMJ Oncol. 2023;2:e000090.
3. Boudoulas KD, Triposkiadis F, Gumina R, Addison D, Iliescu C, Boudoulas H. Cardiovascular disease, cancer, and multimorbidity interactions: clinical implications. Cardiology. 2022;147:196-206.
4. De Boer RA, Meijers WC, Van Der Meer P, Van Veldhuisen DJ. Cancer and heart disease: associations and relations. Eur J Heart Fail. 2019;21:1515-25.
5. Battistoni A, Volpe M. Recent warnings about antihypertensive drugs and cancer risk: where do they come from? Eur Cardiol. 2020;15:e16.
6. Zuin M, Nohria A, Henkin S, Krishnathasan D, Sato A, Piazza G. Pulmonary embolism-related mortality in patients with cancer. JAMA Netw Open. 2025;8:e2460315.
7. Gardezi SA, Sachdeva N, Rampurawala IM, et al. Trends and disparities in inflammatory bowel disease and cardiovascular disease-related mortality in the United States from 1999 to 2023: A CDC WONDER analysis. Int J Cardiol Cardiovasc Risk Prev. 2025;26:200438.
8. Kumar A, Khadke S, Alkindi S, et al. Particulate matter 2.5 pollution impact on comorbid cancer and cardiovascular disease mortality in the U.S. JACC Adv. 2024;3:101106.
9. Ahmed M, Javaid H, Shafiq A, et al. Trends and disparities in coronary artery disease and obesity‐related mortality in the united states from 1999-2022. Endocrino Diabet Metabol. 2024;7:e70010.
10. Ansari HUH, Mahboob E, Samad MA, et al. Temporal trends and disparities in atherosclerosis-associated cerebrovascular disease mortality in the United States, 1999-2020. Curr Probl Cardiol. 2025;50:102935.
11. National intercensal datasets: 2000-2010. Available from: https://www.census.gov/data/datasets/time-series/demo/popest/intercensal-2000-2010-national.html [Last accessed on 20 May 2026].
12. Kim H, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19:335-51.
13. Rakisheva A, Farmakis D, Attanasio A, et al. Prevention of cancer therapy-related cardiac dysfunction and heart failure in cancer patients and survivors. A Clinical Consensus Statement of the Heart Failure Association, the European Association of Preventive Cardiology of the ESC, and the ESC Council of Cardio-Oncology. Eur J Heart Fail. 2025;27:2084-99.
14. Thuny F, Naidoo J, Neilan TG. Cardiovascular complications of immune checkpoint inhibitors for cancer. Eur Heart J. 2022;43:4458-68.
15. Wilcox NS, Amit U, Reibel JB, Berlin E, Howell K, Ky B. Cardiovascular disease and cancer: shared risk factors and mechanisms. Nat Rev Cardiol. 2024;21:617-31.
16. Moslehi JJ. Cardiovascular toxic effects of targeted cancer therapies. N Engl J Med. 2016;375:1457-67.
17. Song S, Guo C, Wu R, et al. Impact of the COVID-19 pandemic on cardiovascular mortality and contrast analysis within subgroups. Front Cardiovasc Med. 2024;11:1279890.
18. Koo TH. Trends and disparities of diverticular disease mortality in the United States before and during the COVID-19 era: estimates from the Centers for Disease Control WONDER database. Ann gastroenterol. 2025;38:428-39.
19. Ebert BL, Libby P. Clonal hematopoiesis confers predisposition to both cardiovascular disease and cancer: a newly recognized link between two major killers. Ann Intern Med. 2018;169:116-7.
20. Ng M, Dai X, Cogen RM, et al. National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050. Lancet. 2024;404:2278-98.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.