



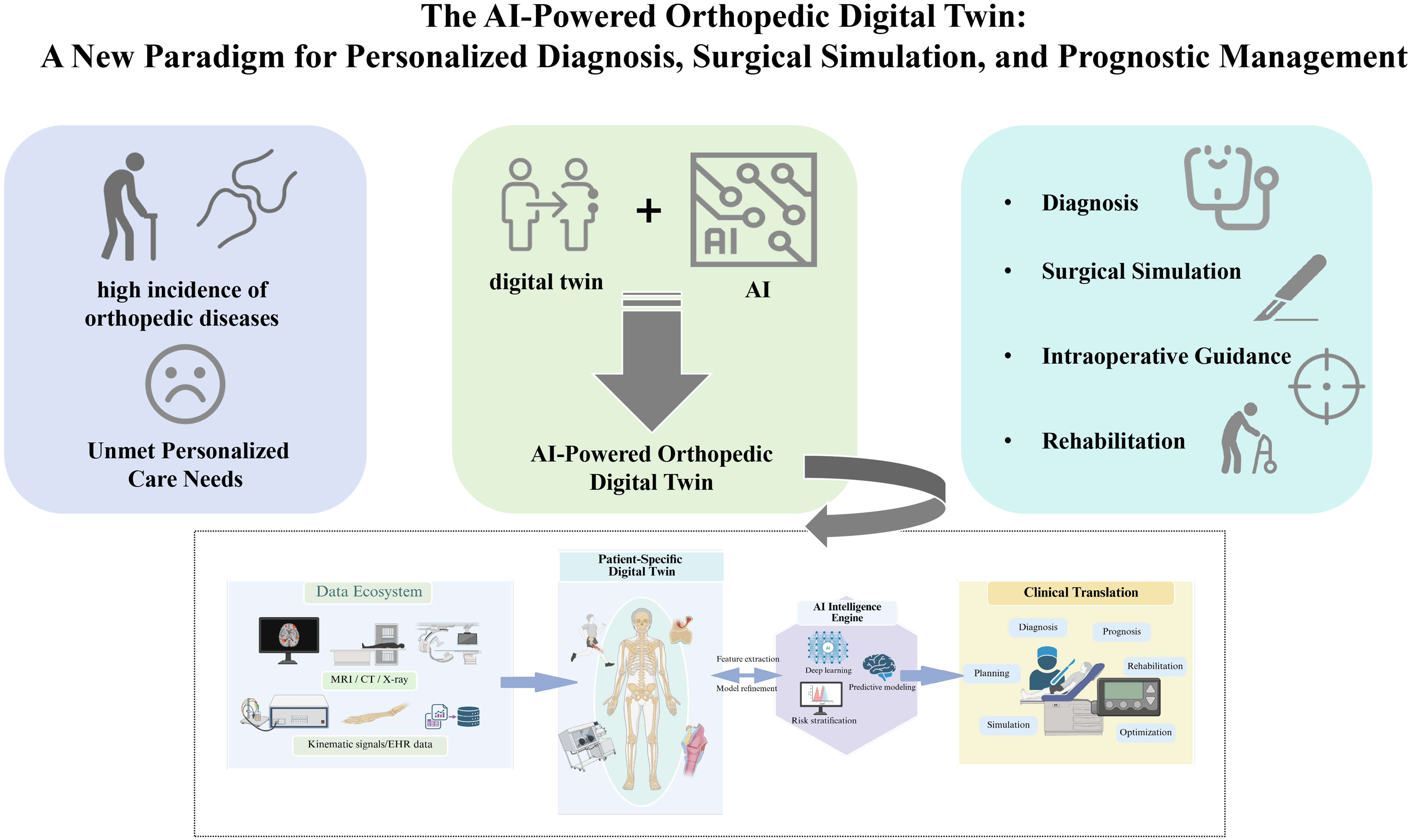
The AI-powered orthopedic digital twin: a new paradigm for personalized diagnosis, surgical simulation, and prognostic management - a scoping review
 0
0 Abstract
Musculoskeletal disorders represent a leading cause of chronic pain and long-term disability worldwide, with conventional orthopedic practices often limited by one-size-fits-all management strategies. This scoping review maps the current landscape of evidence on artificial intelligence (AI)-integrated digital twin (DT) systems in orthopedics, focusing on their conceptual frameworks, clinical applications in personalized diagnosis, surgical simulation and prognostic management, and existing translational gaps. A systematic literature search was conducted across six electronic databases (PubMed, Embase, Web of Science, IEEE Xplore, ACM Digital Library and Scopus) up to 10 February 2026. Fourteen studies published between 2021 and 2026 met the inclusion criteria, with data charted across four predefined core dimensions: patient-specific DT construction, AI-driven biomechanical modeling, diagnostic stratification and surgical simulation, and individualized prognostic modeling. Accumulating preliminary evidence indicates that AI enables orthopedic DTs to evolve from static anatomical replicas to semi-dynamic predictive frameworks, with proof-of-concept applications validated across joint arthroplasty, spinal rehabilitation, foot and ankle surgery, and trauma care. The convergence of AI and DT technologies suggests preliminary technical feasibility and promising translational potential for personalized orthopedic care. However, the field remains in an early translational phase, limited by small sample sizes, single-center designs, insufficient large-scale clinical validation, and heterogeneous methodologies. Further multicenter clinical trials and standardized construction pipelines are required to confirm the clinical effectiveness, safety, and generalizability of AI-powered DT systems in routine orthopedic practice.
Keywords
INTRODUCTION
Musculoskeletal disorders (MSDs) are among the leading causes of chronic pain and long-term physical disability worldwide, imposing a substantial socioeconomic burden that is further exacerbated by population aging[1-5]. Conventional orthopedic practices are limited in their ability to accommodate individual variability, often resulting in suboptimal surgical outcomes, unpredictable recovery trajectories, and increased revision rates[3-7]. Consequently, there is a growing clinical demand for more proactive, predictive, and individualized orthopedic care.
A digital twin (DT) is a virtual representation of a physical entity or process that is continuously informed by real-world data[8-12]. The applications of DTs in healthcare have gained increasing attention in recent years[13-18]. Artificial intelligence (AI) provides a computational intelligence layer that enables DT systems to evolve from static digital representations into adaptive, predictive, and continuously learning clinical models[19-24]. Orthopedics constitutes a particularly suitable clinical domain for DT applications, given its well-defined anatomical structures, established biomechanical principles, and the growing availability of longitudinal imaging and functional data. However, existing orthopedic DT models often fail to incorporate patient-specific variations and dynamic temporal changes, limiting their clinical adaptability[25-29]. Compounding this challenge is the inconsistent use of the term “digital twin” across the orthopedic literature: many studies label static anatomical or biomechanical replicas as digital twins despite the absence of core DT features such as continuous bidirectional data updating. To address this terminological heterogeneity and support structured evidence synthesis, we propose a three-level maturity framework for AI-augmented orthopedic DT systems as an analytical tool for this scoping review, grounded in the widely recognized developmental trajectory of medical digital twins described in prior scoping reviews[10,12,25]: Level 1: Foundational Proto-Digital Twins: Patient-specific static anatomical or biomechanical models constructed from cross-sectional imaging data, without real-time data updating capabilities. These models serve as the core structural building blocks for mature digital twin systems; Level 2: Semidynamic Predictive DT Frameworks: Patient-specific models integrated with AI algorithms for outcome prediction and scenario simulation, with intermittent data updating capacity but no continuous bidirectional data exchange with the physical entity. Level 3: Closed-loop real-time digital twins: Fully functional dynamic virtual replicas that maintain continuous, bidirectional data flow with their physical counterparts, enabling real-time model adaptation and closed-loop clinical decision support. The integration of AI enables DTs to move beyond purely descriptive representations, transforming them into dynamic, predictive, and personalized clinical decision-support systems capable of informing diagnosis, surgical planning, and postoperative management[30-33].
A prior study demonstrated successful translational validation of DT technologies in cardiovascular medicine, where multimodal data were integrated into mechanistic and AI-driven models to personalize diagnosis, optimize interventions, and improve prognostic assessment[34]. Similarly, AI-DT frameworks have shown translational value in thoracic medicine, exemplified by the Lung-DT system that integrates wearable sensor data streams with deep learning algorithms to enable real-time, multimodal respiratory health monitoring and disease characterization[35]. These advances highlight the translational potential of converged AI-DT systems[35-41]; however, their translation to MSDs presents distinct challenges, including the integration of motion dynamics, mechanical loading, and surgery-specific simulation data.
Accordingly, this scoping review aims to map and synthesize the current landscape of AI-powered orthopedic DT systems by (1) describing how patient-specific digital twins are constructed and updated using multisource data; (2) examining how AI methods are embedded to support diagnosis, prediction, and clinical decision-making; (3) summarizing current clinical applications in surgical planning, simulation, and rehabilitation; and (4) discussing key translational challenges and future research directions.
METHODS
This scoping review aims to synthesize the current state of evidence on AI-integrated digital twin systems in orthopedics, with a focus on their technical development, clinical applications, and translational barriers. The study was designed in accordance with the methodological framework for scoping reviews established by Arksey and O’Malley and refined by Levac et al.[42,43], with reporting aligned with the PRISMA Extension for Scoping Reviews (PRISMA-ScR)[44]. The completed PRISMA-ScR checklist is available in Supplementary File 1. A systematic literature search was performed to identify relevant studies, with a predefined framework for qualitative scoping evidence synthesis[45]. The protocol for this review was not pre-registered in a public registry, as the study was designed as a rapid evidence mapping of an emerging, fast-evolving technical field. Dual independent reviewer screening and standardized data charting were implemented to minimize selection bias and ensure reproducibility of literature identification. Consistent with the core aims of scoping reviews to map the breadth of evidence rather than evaluate intervention effectiveness, formal risk-of-bias assessment and quality appraisal of included studies were not performed.
Search strategy
A literature search was conducted in six electronic databases, including PubMed, Embase, Web of Science, IEEE Xplore, ACM Digital Library and Scopus, from inception to 10 February 2026. The core search terms included combinations of “artificial intelligence”, “digital twin”, “orthopedics”, “musculoskeletal disorders”, “personalized diagnosis”, “surgical simulation”, “surgical planning”, and “rehabilitation management”. Boolean operators were used to combine keywords and optimize search sensitivity, with database-specific syntax adapted for each platform. Additionally, we manually screened the reference lists of all the retrieved studies and relevant domain reviews to identify any additional eligible literature. Full search strategies for all six databases are provided in Supplementary File 2.
Study eligibility criteria
Studies were included if they met the following criteria: (1) they focused on the integration of AI algorithms with DT technologies in orthopedic clinical contexts; (2) they reported technical, clinical, biomechanical, or patient-related outcomes relevant to orthopedic diagnosis, surgical planning, simulation, rehabilitation, or prognostic management; and (3) they were full-length, peer-reviewed journal articles or full conference papers published in English. To provide a comprehensive landscape of this rapidly evolving field, we included: (a) original clinical validation studies and methodological development research; (b) conceptual studies proposing original technical or architectural frameworks specific to AI-integrated orthopedic DTs; (c) high-quality methodological reviews establishing standardized construction pipelines for musculoskeletal DT systems.
Studies were excluded if they met the following criteria: (1) were duplicate publications; (2) were editorials, letters to the editor, theses, conference abstracts, general narrative reviews, expert commentaries or opinion pieces without original conceptual frameworks or methodological contributions to orthopedic DT systems; (3) were not published in English; and (4) focused on AI or DT applications in nonorthopedic fields.
Study selection and data charting
All titles and abstracts of the studies were downloaded and imported into the reference management program Endnote X9, and all duplicates were removed through the software’s built-in functions and manual checks. Two independent reviewers performed title/abstract screening and full-text eligibility assessment in duplicate, independently and in parallel. Disagreements were resolved via consensus discussion or arbitration by a third senior reviewer. Two independent reviewers also performed data charting in duplicate using a predefined, standardized data charting form, which included the following information: first author, publication year, specific clinical scenario and technical application of AI-integrated DT systems, DT maturity level (classified by the author-proposed three-level framework), study design type, and key study outcomes. Disputes were settled through dialog or by seeking the opinion of a third reviewer.
To address the clinical and methodological heterogeneity of the included studies[46], we predefined a structured synthesis framework across four core dimensions prior to the literature screening and data charting: (1) conceptual architecture and construction methods of musculoskeletal digital twins; (2) AI-driven diagnosis and clinical decision support; (3) surgical simulation, planning and intraoperative optimization; and (4) prognostic prediction and personalized rehabilitation management. Data from the included studies were charted and synthesized according to this framework, with key limitations of each study and the overall evidence base systematically documented.
Consistent with scoping review methodology to capture the full breadth of an emerging research field, we adopted this broad inclusion scope to map the complete developmental landscape of AI-powered orthopedic DT research. We included studies across the entire translational pipeline (from methodological development and conceptual frameworks to preclinical validation and early clinical trials) to provide a comprehensive overview of current progress. Evidence from different study types is stratified and interpreted with corresponding caution in the synthesis.
Characteristics of included studies
A total of 420 publications were initially identified through database searches and supplementary manual screening of reference lists. A total of 139 duplicates were removed, resulting in 281 unique records for the title and abstract screening. Following this, 261 articles were excluded because they focused on AI or DT applications in fields other than orthopedics. Ultimately, 20 studies underwent full-text assessment, of which 14 met all the inclusion criteria and were included in the final synthesis. All included studies were published between 2021 and 2026. The search processes are shown in Figure 1.
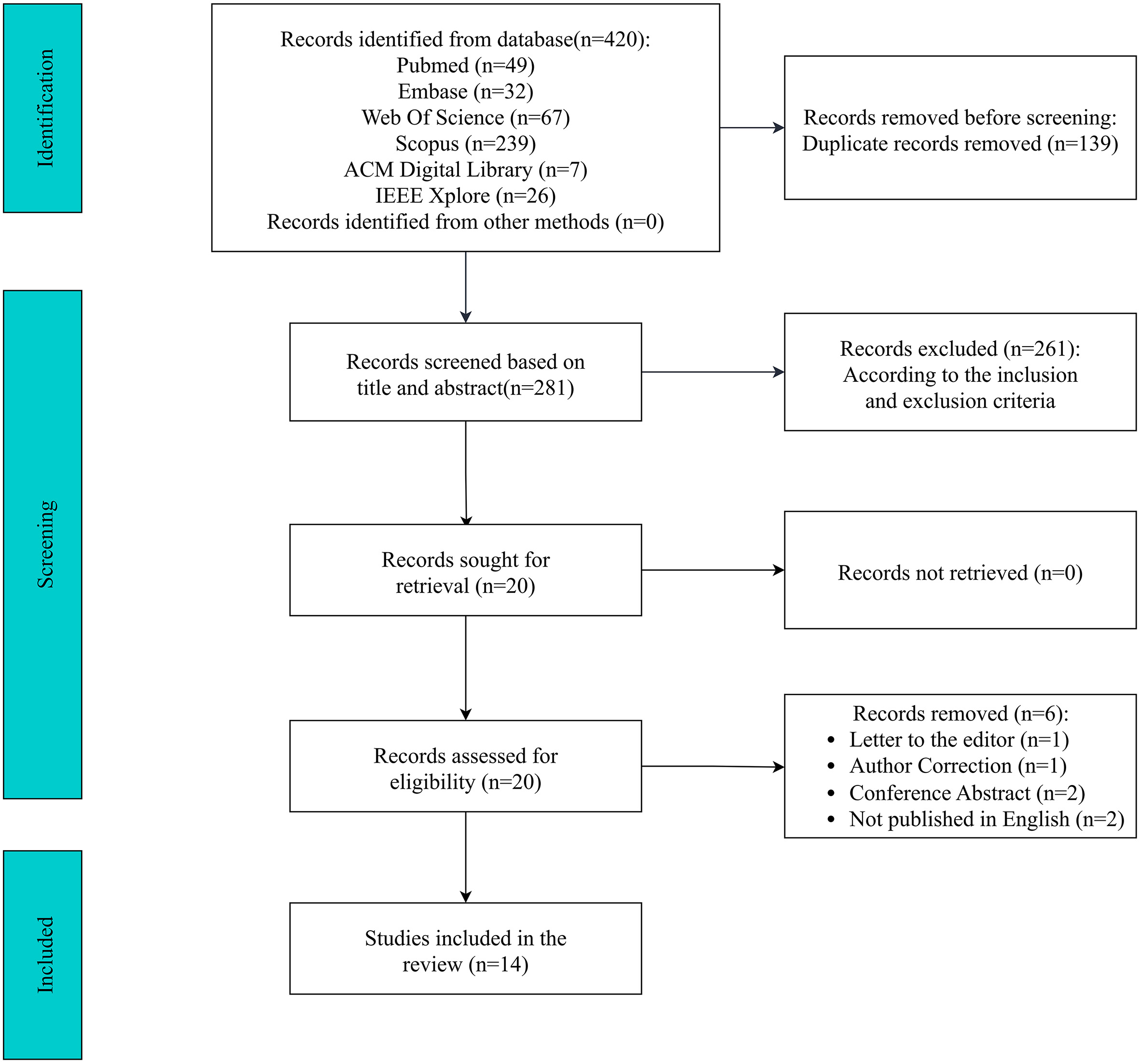
Figure 1. The search and selection processes.
The 14 included studies can be stratified into four categories by study type: 5 technical development studies focused on model construction methodology, 4 preclinical validation studies testing model performance in simulated or ex vivo settings, 3 conceptual/framework studies proposing architectural or methodological standards, 1 clinical trial investigating patient-reported and functional outcomes, and 1 health services research study analyzing operating room workflow efficiency. This distribution reflects the early translational stage of the field, with most work concentrated on technical proof-of-concept rather than large-scale clinical effectiveness evaluation.
The characteristics of the 14 included studies are reported in Table 1. To better characterize the functional orientation of the included studies, we mapped all the studies to the four predefined analytical dimensions outlined in the Methods section: (1) DT construction; (2) AI-enhanced predictive modeling; (3) surgical simulation; and (4) rehabilitation-oriented decision support. Notably, most studies spanned multiple dimensions, reflecting the intrinsically integrative nature of AI-powered orthopedic DT systems. A conceptual overview of AI-powered digital twin systems in orthopedics is shown in Figure 2.
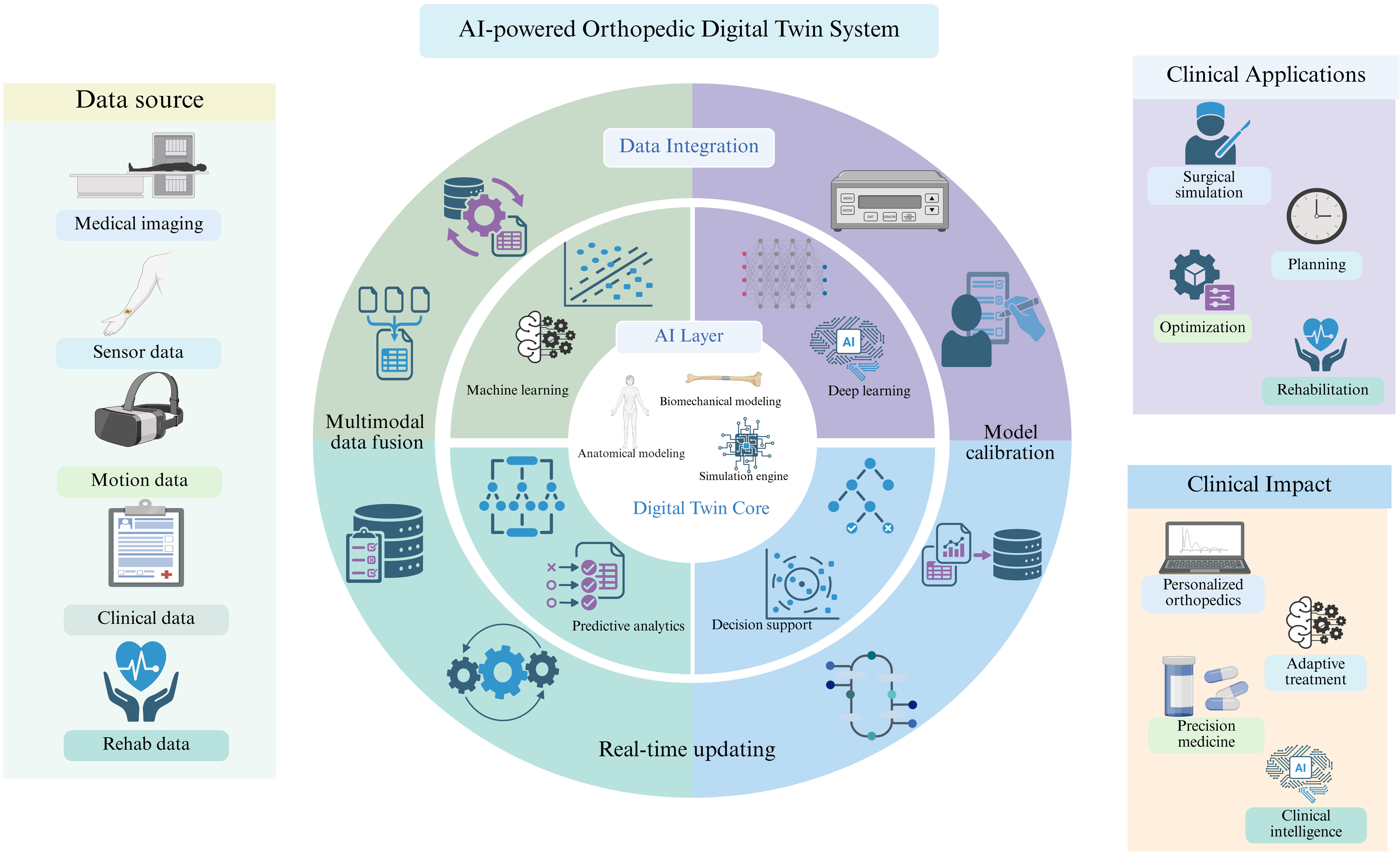
Figure 2. Conceptual overview of AI-powered digital twin systems in orthopedics. Multimodal patient data are integrated into dynamic digital twin models and enhanced by AI-driven analytics to support diagnosis, prediction, surgical planning, and rehabilitation. The system enables adaptive, personalized, and data-driven clinical decision-making in precision orthopedics. Created in BioRender. Wu, H. (2026) https://BioRender.com/0ngyql5. AI: Artificial intelligence.
Characteristics of the representative studies included in this review
| Title | First author | Year of publication | Specific applications of DT and AI in orthopedics | DT maturity level | Study design |
| Digital twins, artificial intelligence, and machine learning technology to identify a real personalized motion axis of the tibiotalar joint for robotics in total ankle arthroplasty | Hernigou[47] | 2021 | Identifies a patient-specific ankle motion axis via DT and AI for planning and guiding robotic total ankle arthroplasty | Level 1 (Foundational Proto-DT) | Technical development/biomechanical modeling study |
| Foundations of a knee joint digital twin from qMRI biomarkers for osteoarthritis and knee replacement | Hoyer[49] | 2025 | Constructs a knee joint DT using qMRI biomarkers and AI to predict osteoarthritis incidence and knee replacement outcomes | Level 1 (Foundational Proto-DT) | Retrospective imaging-based predictive study |
| Surgical digital twin reconstruction from tool tracking - lecture notes in computer science | Stauffer[55] | 2026 | Dynamically reconstructs a surgical DT via tool tracking and AI (e.g., LSTM) to enable real-time implant integration and surgical guidance | Level 2 (Semidynamic Predictive DT Framework) | Technical development/algorithm validation study |
| A practical guide to the implementation of AI in orthopedic research - part 1: opportunities in clinical application and overcoming existing challenges | Zsidai[75] | 2023 | Establishes a standardized methodological framework for musculoskeletal DT construction integrating multisource data, and defines core requirements for AI-enhanced diagnosis, simulation, and clinical decision-making | Conceptual Methodological Framework | Methodological review/conceptual framework |
| A five-dimensional three-layer digital twin to train a reinforcement learning agent for interaction control of a robotic exoskeleton in adolescent idiopathic scoliosis rehabilitation | Farhadiyadkuri[48] | 2025 | Provides a 5D DT simulation environment to train a Reinforcement Learning agent for optimizing control of a robotic exoskeleton in scoliosis rehabilitation | Level 2 (Semidynamic Predictive DT Framework) | Simulation-based technical development study |
| Subtalar axis determined by combining digital twins and artificial intelligence: influence of the orientation of this axis for hindfoot compensation of varus and valgus knees | Hernigou[54] | 2022 | Determines a patient-specific subtalar joint axis using DT and AI to analyze hindfoot compensation mechanisms for personalized diagnosis and planning | Level 1 (Foundational Proto-DT) | Biomechanical analysis study |
| Ankle and foot surgery: from arthrodesis to arthroplasty, three dimensional printing, sensors, artificial intelligence, machine learning technology, digital twins, and cell therapy | Hernigou[107] | 2021 | A conceptual article describing the potential of DT and AI for personalized kinematic analysis and robotic surgical planning in foot and ankle surgery | Conceptual Perspective | Narrative perspective/conceptual review |
| Construction method and application of human skeleton digital twin | Song[56] | 2022 | Proposes a method to construct a human skeleton DT for real-time biomechanical monitoring, using AI surrogate models for prediction | Level 2 (Semidynamic Predictive DT Framework) | Technical development/case validation study |
| Shared decision making using digital twins in knee osteoarthritis care: a randomized clinical trial of an AI-enabled decision aid versus education alone on decision quality, physical function, and user experience | Jayakumar[52] | 2025 | Employs AI to generate patient-specific "digital twins" providing personalized outcome predictions to augment shared decision-making in knee OA care | Level 2 (Semidynamic Predictive DT Framework) | Randomized controlled clinical trial |
| Toward an artificial intelligence-assisted framework for reconstructing the digital twin of vertebra and predicting its fracture response | Ahmadian[50] | 2022 | Proposes an AI-assisted framework (ReconGAN) to reconstruct a patient-specific vertebral DT integrating microstructure for fracture risk prediction and biomechanical simulation | Level 1 (Foundational Proto-DT) | Technical development/finite element validation study |
| Optimizing operating room efficiency in robotic-assisted total knee arthroplasty through manufacturing efficiency principles | Hiraoka[83] | 2025 | Utilizes a DT to simulate and analyze OR workflow, applying lean manufacturing principles and AI-driven data analysis to optimize efficiency in robotic TKA | Level 2 (Semidynamic Predictive DT Framework) | Retrospective operational analysis study |
| Malalignment detection in TKA: a digital twin framework using instrumented tibial trays | Merzak[53] | 2025 | Develops a DT framework integrated with neural networks to detect prosthesis malalignment in TKA via strain signal analysis | Level 2 (Semidynamic Predictive DT Framework) | Technical development/in vitro validation study |
| Replication of impedance identification experiments on a reinforcement-learning-controlled digital twin of human elbows | Yu[51] | 2024 | Replicates elbow impedance identification experiments using a reinforcement learning-controlled human elbow DT for validating rehabilitation techniques. | Level 2 (Semidynamic Predictive DT Framework) | Simulation-based algorithm validation study |
| Biomechanics digital twin: markerless joint acceleration prediction using machine learning and computer vision | Leal[108] | 2023 | Constructs a biomechanical DT with machine learning and computer vision for markerless joint acceleration prediction and injury risk prevention | Level 2 (Semidynamic Predictive DT Framework) | Technical development/observational validation study |
CONCEPTUAL ARCHITECTURES OF MUSCULOSKELETAL DIGITAL TWINS
To structurally synthesize the diverse design paradigms, data flows, and application models identified across the included studies, we propose an integrated conceptual architectural framework that synthesizes common elements across existing studies, conceptualizing AI-powered orthopedic digital twin systems as closed-loop, multilayered structures (detailed in Figure 3). This framework is a synthesized analytical model developed by the authors based on the included evidence, rather than a pre-existing architecture reported in a single included study.
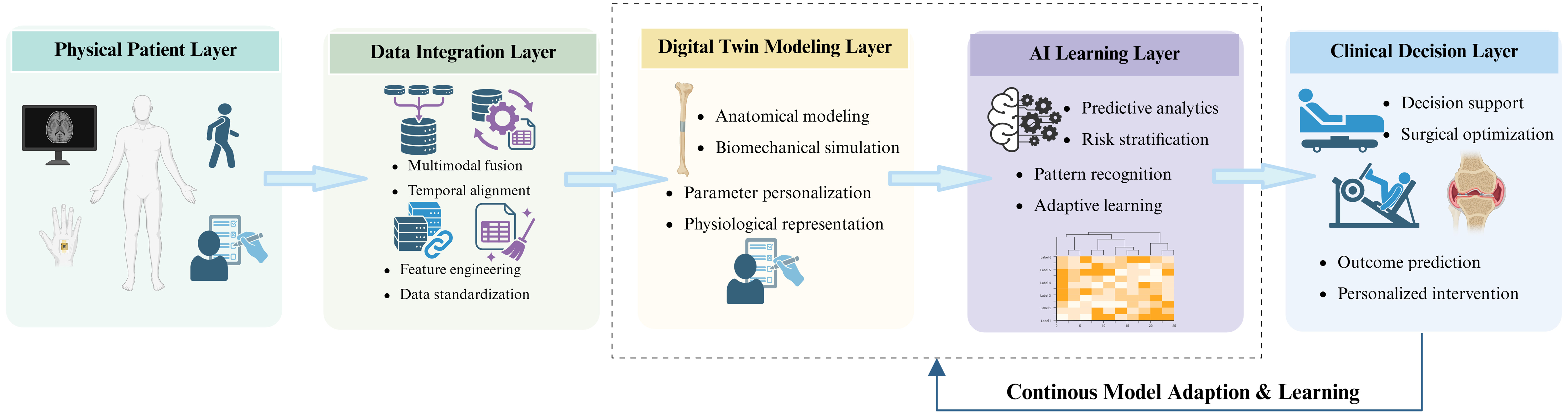
Figure 3. Integrated architecture of AI-powered orthopedic DT systems. Created in BioRender. Wu, H. (2026) https://BioRender.com/pbglri8. AI: Artificial intelligence; DT: digital twin.
This closed-loop, multilayered framework operates through continuous bidirectional data flow across five interdependent layers: (1) Physical Patient Layer: the real-world clinical entity that serves as the source of all the raw data and the end target of clinical interventions; (2) Data integration layer: This layer standardizes, temporally aligns, and fuses multimodal heterogeneous data streams, including medical imaging, biomechanical motion signals, electronic health records, and wearable sensor data, to support downstream modeling; (3) Digital Twin Modeling Layer: This layer involves the construction of patient-specific anatomical and biomechanical models from integrated data, providing the structural and mechanistic foundation of the system; (4) The AI learning layer performs feature extraction, pattern recognition, outcome prediction, and adaptive parameter optimization, endowing the digital twin with predictive intelligence and dynamic updating capacity; (5) Clinical Decision Layer: This layer translates model outputs into actionable clinical decision support, including diagnostic risk stratification, surgical plan optimization, and personalized intervention recommendations. The outer closed loop enables continuous model adaptation and learning from new clinical data.
The construction of patient-specific musculoskeletal DTs relied on the integration of multisource heterogeneous data. Current methodologies range from geometry-driven biomechanical models to data-driven generative frameworks, each addressing different aspects of fidelity and complexity.
Hernigou et al.[47] demonstrated the use of CT-based 3D bone models converted into mathematical objects using CAD software (CatiaTM) to identify a patient-specific motion axis of the tibiotalar joint, forming the basis for robotic surgical planning. However, this approach was limited by the use of a small sample (5 real + 20 DTs) and did not account for dynamic soft-tissue influences. It also relies on specialized and costly CAD software, which limits its clinical accessibility.
Farhadiyadkuri and Zhang[48] proposed a comprehensive five-dimensional three-layer DT architecture (the five dimensions refer to the physical patient entity, the virtual simulation model, the centralized twin data repository, the bidirectional data connection between physical and virtual layers, and the clinical service application layer) emphasizing bidirectional data flow (physical-to-virtual and virtual-to-physical). Their framework successfully created a high-fidelity patient-specific musculoskeletal DT, although it simplified the human torso as a single solid body and relied on a limited dataset for parameter identification.
Hoyer et al.[49] constructed a Level 1 foundational knee joint proto-DT using quantitative MRI biomarkers and employed deep learning-based segmentation and principal component analysis (PCA) to create an interpretable feature space for predicting osteoarthritis (OA) incidence and knee replacement outcomes. However, PCA captured limited variance for some biomarkers (45%-65%), and model generalizability across diverse populations remained unvalidated.
Ahmadian et al.[50] introduced ReconGAN, a 3D deep convolutional generative adversarial network (DCGAN) framework, to synthesize realistic trabecular bone microstructures from microQCT images. This approach enabled the creation of a biomechanically realistic vertebral DT for fracture risk prediction, although it depended on a limited and nondiverse training dataset.
Yu et al.[51] developed a reinforcement learning-driven neuromechanical DT of the human elbow, demonstrating the feasibility of AI-controlled digital humans as functional DT entities for biomechanical experimentation.
Collectively, these studies indicate that musculoskeletal DT construction is evolving from purely geometry-driven models to hybrid approaches in which AI supports high-resolution structural synthesis and parameter estimation, while biomechanical principles preserve physical plausibility.
AI-DRIVEN DIAGNOSIS AND DECISION-MAKING
AI algorithms, particularly deep learning and multivariate statistical models, have been embedded within DT frameworks to enable early diagnosis, risk stratification, and individualized treatment planning[26].
Hoyer et al.[49] leveraged deep learning-based segmentation and PCA-derived imaging biomarkers to construct predictive models for OA progression and knee replacement. Their analysis revealed protective factors and risk factors. Although these models offer a more nuanced understanding of joint degeneration trajectories, their clinical utility still depends on radiological expertise and lacks external validation.
Jayakumar et al.[52] conducted a randomized clinical trial evaluating an AI-enabled decision aid (AI-DA) that generated patient-specific predictive models of outcomes after different treatment options for knee OA. Compared with education alone, AI-DA use resulted in higher decision quality, lower decisional regret, and improved functional outcomes at 6-9 months. Nevertheless, the “black-box” nature of the AI and potential algorithmic biases were acknowledged as important limitations.
Merzak et al.[53] demonstrated neural network-based virtual sensing within implant-integrated digital twins for prosthesis malalignment detection, illustrating the emergence of DT-enabled autonomous diagnostic mechanisms.
Overall, the included studies illustrate that integrating AI within DTs can extend musculoskeletal care from static imaging-based diagnosis to dynamic, data-driven risk prediction and personalized decision support.
SURGICAL SIMULATION AND OPTIMIZATION
DTs augmented with AI have shown potential to enable preoperative simulation, surgical planning, and intraoperative guidance.
Hernigou et al.[47,54] described a personalized joint axis defined in a geodesic coordinate system, allowing robotic systems to perform precise bone cuts in total ankle arthroplasty. However, the clinical translation of this method requires validation in live robotic surgery and assumes rigid bone behavior.
Stauffer et al.[55] proposed a method to indirectly integrate surgical implants (plates and screws) into DTs by analyzing tool-bone interactions using deterministic drilling detection and an LSTM network for screw classification. Their approach achieved a 96.4% screw and 100% plate detection rate, enabling dynamic implant integration with high geometric fidelity (Screw RMSE 1.52 mm, Plate RMSE 0.94 mm). Limitations included susceptibility to marker occlusion and the fact that plate reconstruction initiates only after the third screw, delaying feedback.
Farhadiyadkuri and Zhang[48] trained a reinforcement learning-based impedance controller within a 5D DT to optimize the interaction of a robotic exoskeleton for scoliosis rehabilitation. The controller demonstrated superior tracking and force control in simulation, although real-world clinical validation is pending.
Taken together, these studies underscore the promise of AI-powered DTs in closing the loop between preoperative planning and intraoperative execution, particularly in robotic and navigation-assisted procedures. However, most systems operate in an offline or semistatic fashion, with limited integration of live physiological or kinematic data, and no large-scale clinical trials have confirmed the intraoperative safety and effectiveness of these systems.
PROGNOSTIC PREDICTION AND REHABILITATION MANAGEMENT
Several studies have showcased the use of DTs, often augmented by AI, for prognostic prediction, postoperative monitoring, and personalized rehabilitation.
Jayakumar et al.[52] reported that AI-DA-generated DTs led to better long-term functional outcomes and higher treatment concordance in patients with knee OA who underwent total knee arthroplasty (TKA). This work provides early clinical evidence that DT-based predictions can influence both decision-making and real-world recovery.
Song et al.[56] implemented a real-time human skeleton DT for the biomechanical monitoring of lumbar spine stress during various postures. The system was validated in a human lumbar spine case using motion capture and finite element modeling, although clinical validation in rehabilitation settings is still needed.
Ahmadian et al.[50] used their vertebral DT to simulate fracture response under different loading conditions, revealing ductile versus brittle failure modes based on load type and tumor presence. These insights could inform postoperative management and preventive strategies, although the model does not yet incorporate real-time data updates.
Collectively, these findings indicate that DTs have considerable promise for dynamic prognostic modeling and rehabilitation planning. Nonetheless, most current implementations are based on one-time simulations rather than continuously updated, real-time digital replicas of the patient.
SUMMARY OF INCLUDED STUDIES
This review synthesizes recent advances in AI-powered DT technologies in orthopedics on the basis of current published evidence. Collectively, findings from the included studies suggest the growing technical feasibility of integrating multimodal patient data and computational modeling into unified DT systems to support personalized orthopedic care[57-60].
Beyond technical integration, these developments indicate a conceptual transition of orthopedic digital twins from static digital replicas toward individualized and adaptive digital representations. This conceptual transition suggests a shift in DTs from passive modeling tools toward more adaptive and intelligent clinical support systems capable of supporting dynamic decision-making and personalized intervention planning.
Digital twin construction: reconciling mechanistic and data-driven paradigms
The foundational step in developing musculoskeletal DTs is the integration of multisource, heterogeneous data to create high-fidelity, patient-specific virtual models[61]. Current approaches reveal a fundamental dichotomy between mechanistic (physics-based)[62,63] and data-driven (AI-based)[64] modeling paradigms.
Studies such as those by Hernigou et al.[47] and Farhadiyadkuri and Zhang[48] exemplified the mechanistic approach of using CAD and engineering software to create geometrically and biomechanically precise models. Their strengths lie in interpretability and principled generalization based on biomechanical and physical laws. However, they often rely on costly software, require expert knowledge, and struggle to model complex biological heterogeneity[65-67].
In contrast, the work of Hoyer et al.[49] and Ahmadian et al.[50] represented a data-driven paradigm, employing deep learning to extract patterns and generate structures directly from imaging data. This approach excelled at capturing complex, nonlinear relationships but resulted in “black-box” models whose generalizability is limited by the quality and diversity of their training data[68-70].
The development of high-fidelity musculoskeletal DTs[71] is likely to depend on hybrid frameworks that tightly couple mechanistic and AI-based components. In such systems, AI modules would be constrained by biomechanical priors and physical laws, whereas mechanistic models would be dynamically personalized through AI-driven parameter estimation and real-time data assimilation.
AI-enhanced diagnosis and decision-making: toward precision orthopedics
AI has shown significant potential for improving diagnostic accuracy, particularly in risk stratification, and enhancing prognostic forecasting[72-74].
The model developed by Hoyer et al.[49] successfully identified imaging biomarkers for early osteoarthritis and predicted fracture risk with high accuracy, which indicates a potential shift from diagnosing established pathologies toward forecasting individualized risk trajectories. However, the current work remains limited by the use of single-center datasets, incomplete representation of diverse patient populations, and a lack of external validation.
Notably, AI-DAs, as implemented by Jayakumar et al.[52], could synthesize patient-specific data to improve shared decision-making and postoperative outcomes. These tools represent a step beyond traditional population-based risk calculators toward more personalized, individual-level clinical decision-making. A significant barrier to this vision, as highlighted across studies by Zsidai et al.[75], was the “black-box” nature of many advanced AI models, which compromises clinical interpretability[76].
Therefore, the next generation of AI-integrated orthopedic DT systems must become interpretable decision-support partners[74,77-82]. This requires systems (1) to visualize and track the evolution of key biomarkers and biomechanical parameters over time; (2) to link diagnostic findings to probable long-term outcomes under different treatment strategies; and (3) to translate complex model outputs into concise evidence for shared decision-making.
Surgical simulation and optimization: From planning to execution
DTs offer a powerful platform for preoperative planning and surgical simulation, allowing surgeons to visualize patient-specific anatomy, predict biomechanical outcomes, and optimize intervention strategies. Studies by Hernigou et al.[47] and Stauffer et al.[55] illustrated the potential of DTs in guiding robotic surgery and intraoperatively tracking implant placement. These applications have shown preliminary potential to improve surgical precision, reduce operative time, and extend implant longevity in preclinical and small-sample validations, although these theoretical benefits have not been confirmed in large-scale randomized controlled trials.
However, most current surgical DTs are static and cannot adapt intraoperatively on the basis of live physiological feedback. The study by Hiraoka et al.[83], while focused on process efficiency, underscores the broader potential of DTs to optimize surgical workflows.
A key priority for future research is the development of adaptive surgical DT systems operating within real-time closed-loop “sense-simulate-guide” frameworks, with robust clinical validation to confirm safety and effectiveness in live surgical settings[84-86]. In this paradigm, intraoperative data (e.g., from fluorescence imaging) dynamically update the DT[87]. An AI-driven module would then perform rapid simulations to predict the biomechanical consequences of various surgical options. Finally, optimized guidance is delivered to the surgeon via augmented reality (AR) or robotic interfaces, completing the loop from data acquisition to surgical action[88,89].
Key research challenges toward realizing this vision include real-time modeling of soft-tissue mechanics, ultrafast edge-based biomechanical simulations, and the establishment of robust human-machine interaction (HMI) protocols to guarantee clinical safety[90].
Prognostic prediction and rehabilitation: enabling dynamic postoperative management
Postoperatively, DTs combined with AI can dynamically predict recovery trajectories and complication risks, guiding personalized rehabilitation[91-94]. Studies by Song et al.[56] and Ahmadian et al.[50] have demonstrated how biomechanical DTs can simulate load responses and predict failure modes, informing rehabilitation strategies and preventive interventions. Beyond degenerative and traumatic spinal conditions, DT-enabled precision prognostication also holds high translational value for spinal cord injury, where dynamic molecular fibrotic biomarkers can be integrated into prognostic models to stratify individual functional repair trajectories[95]. Jayakumar et al.[52] further reported that predictive DTs can lead to better long-term functional outcomes and higher patient compliance.
However, the transition from static simulation to dynamic, real-time prognostic systems remains a significant hurdle. Current models largely lack integration with real-time continuous patient data, limiting their use in adaptive care pathways. The critical next phase is to create a prognostic system in which the DT is perpetually updated by wearable sensor data (e.g., on activity, gait, and load)[96], patient-reported outcomes, and even subsequent imaging. This DT could then dynamically adjust the rehabilitation goals, predict complications such as implant loosening before they become clinically apparent, and empower patients with visual recovery trajectories.
Challenges and future directions
Despite considerable promise, the widespread clinical implementation of DTs in orthopedics faces several intertwined technical, clinical, and ethical challenges.
Technical and methodological hurdles
Key issues include data fragmentation, model generalizability[97] across diverse populations, high computational costs, and the complexity of integrating real-time data streams[98-100]. Many studies are limited by inherently small sample sizes and retrospective designs. Future work must prioritize prospective, multicenter trials to validate models clinically. Additionally, advancing toward markerless tracking, multisensor fusion, and more efficient computational algorithms will be crucial for real-time applications.
Clinical integration and safety
Integrating DT technologies into existing clinical workflows without disrupting efficiency is a major challenge. Furthermore, deploying AI or DT predictions in high-stakes surgical settings without rigorous validation poses patient safety risks[101]. The development of clear regulatory frameworks, clinical guidelines, and competency standards for DT-augmented care is essential.
Ethical and interpretability concerns
The opacity of complex AI models, data privacy concerns, and potential accountability gaps for AI-driven recommendations are significant barriers to trust. Advancing explainable-AI techniques and addressing equity in access are essential ethical and governance considerations[102-106].
The development of AI-powered DT systems follows distinct trajectories across orthopedic subspecialties, shaped by unique anatomical features and clinical workflow demands[107,108]. In joint arthroplasty, the most established applications center on preoperative planning and implant alignment optimization, with bony geometry forming the core of current proto-DT models; the key challenge here is integrating dynamic soft-tissue and in vivo kinematic data to move beyond static geometry-only planning. In spinal care, DTs are primarily applied to biomechanical stress simulation and robotic exoskeleton control for scoliosis rehabilitation, where unique barriers arise from the complex multisegmental kinematics of the spine and the need for long-term wearable data integration. For traumatic spinal cord injury, another core clinical indication in spinal care, multi-layered pathophysiological alterations from molecular fibrotic regulatory pathways to supraspinal neuroplastic reorganization further elevate the technical requirements for personalized DT construction[109,110]. In foot and ankle surgery, DTs have been leveraged to identify patient-specific joint motion axes for robotic surgical guidance, with the main technical limitation being achieving sufficient spatial precision for small, anatomically complex joint structures. In trauma orthopedics, intraoperative DT reconstruction and implant tracking represent the primary use cases, where the critical challenge is ultrafast model updating to accommodate the time-sensitive nature of emergency surgical settings[111]. Finally, in musculoskeletal rehabilitation, AI-augmented DTs focus on real-time motion monitoring and adaptive rehabilitation prescription, where the principal limitation is the scarcity of longitudinal real-world data to support continuous model calibration.
Collectively, these barriers reflect a systemic translational gap between technical feasibility and scalable clinical deployment.
Limitations
This review has several limitations that should be acknowledged. First, the inclusion criteria were restricted to publications in English, which may have led to the omission of pertinent studies published in other languages, introducing a potential language bias. Second, given the rapid evolution of AI and DT technologies, some very recent developments may not be captured because of the inherent delay in publication and indexing. Third, given the significant heterogeneity in study designs, technical pipelines, and outcome measures across the included studies, a quantitative meta-analysis was not feasible, with all findings presented as a descriptive qualitative synthesis aligned with scoping review methodology. Finally, as the field is nascent, most included studies are early-phase technical validations rather than large-scale clinical effectiveness trials; therefore, the reported technical potential and translational challenges are indicative of the current developmental stage rather than definitive clinical evidence of patient benefit.
CONCLUSION
AI-powered digital twin technologies show promising potential to advance orthopedic research and clinical practice, offering patient-specific solutions across the continuum of diagnosis, surgical planning, rehabilitation, and long-term monitoring. Current research provides converging preliminary evidence supporting the technical feasibility and early translational potential of AI-powered DT systems across multiple orthopedic subfields, from joint arthroplasty to spinal care and rehabilitation.
However, the field remains in an early translational phase, characterized by fragmented methodological standards, limited high-quality clinical validation, and persistent technical and regulatory challenges. The overall evidence base is currently limited to small-scale, single-center studies, with only one randomized controlled trial identified to date. Future efforts should focus on standardizing DT construction pipelines, fostering interoperability across systems, conducting robust multicenter clinical trials to confirm clinical effectiveness and safety, and addressing critical ethical and explainability concerns to support clinical translation.
DECLARATIONS
Acknowledgments
The Graphical Abstract was created with BioRender.com.
Authors’ contributions
Made substantial contributions to the conception and design of the study: Li R, Wang W
Literature screening and data charting: Wu H
Data synthesis and interpretation: Wu H, Tang X
Drafted the original manuscript: Wu H
Critically revised the manuscript for important intellectual content: Tang X, Li R, Wang W
Provided overall supervision: Li R, Wang W
All the authors approved the final version for submission.
Availability of data and materials
The dataset used for the current study is available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
Funding sources for individual included studies were not systematically charted as part of this scoping review. This work was supported by the Shandong Province Natural Science Foundation (Nos. ZR2024MH012, and ZR2023QH321), National Natural Science Foundation of China (No. 82402801), Shandong Provincial Education Department Project (No. 2024KJJ078), Young Talent of Lifting Engineering for Science and Technology in Shandong (No. SDAST2025QTA009), China International Medical Foundation Project (No. Z-2017-24-2509), Open Research Fund of Jiangsu Key Laboratory of Organoid Engineering and Precision Medicine (No. 260PM03), Special Fund of State Key Laboratory of Respiratory Health and Multimorbidity (2060204-2026), and 1·3·5 Project of State Key Laboratory of Respiratory Health and Multimorbidity, West China Hospital, Sichuan University (RHM25210, RHM24101, RHM25101). The funders played no role in the study design, data collection, data analysis, interpretation of results, writing of the manuscript, or the decision to submit the paper for publication.
Conflicts of interest
Wang W is the Guest Editor of the Special Issue “Artificial Intelligence and Digital Twins in Orthopedic Diseases and Bone Regeneration” of Artificial Intelligence Surgery. Wang W was not involved in any stage of the editorial process for this manuscript, including reviewer selection, manuscript handling, or decision-making. The other authors declare that there are no conflicts of interest related to this manuscript.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81:646-56.
2. United Nations Department of Economic and Social Affairs. World population aging 2023: Challenges and opportunities of population ageing in the least developed countries. 2024. Available from https://www.un.org/development/desa/pd/content/launch-World-Population-Ageing-2023 [accessed 26 June 2026].
3. Qiu K, Wang C, Mo X, et al. The global macroeconomic burden of musculoskeletal disorders. Int J Surg. 2025;111:7857-66.
4. Molina-Garcia P, Mora-Traverso M, Prieto-Moreno R, Díaz-Vásquez A, Antony B, Ariza-Vega P. Effectiveness and cost-effectiveness of telerehabilitation for musculoskeletal disorders: a systematic review and meta-analysis. Ann Phys Rehabil Med. 2024;67:101791.
5. Raleigh SM. Genetic and epigenetic factors that predispose to musculoskeletal disorders. Genes. 2024;15:1194.
6. Seixas-Lopes FA, Lopes C, Marques M, Agostinho C, Jardim-Goncalves R. Musculoskeletal disorder (MSD) health data collection, personalized management and exchange using Fast Healthcare Interoperability Resources (FHIR). Sensors. 2024;24:5175.
7. Macdonald WA, Oakman J. Changes needed to reduce risk of musculoskeletal disorders. Am J Ind Med. 2024;67:575-81.
8. Mosquera-Lopez C, Jacobs PG. Digital twins and artificial intelligence in metabolic disease research. Trends Endocrinol Metab. 2024;35:549-57.
10. Katsoulakis E, Wang Q, Wu H, et al. Digital twins for health: a scoping review. NPJ Digit Med. 2024;7:77.
11. Reiche LT, Gundlach CS, Mewes GF, Fay A. The digital twin of a system: a structure for networks of digital twins. In: 2021 IEEE 26th International Conference on Emerging Technologies and Factory Automation (ETFA); 2021 Sep 7-10; Vasteras, Sweden. IEEE; 2021. pp. 1-8.
12. Zhang K, Zhou H, Baptista-Hon DT, et al. Concepts and applications of digital twins in healthcare and medicine. Patterns. 2024;5:101028.
13. Venkatesh KP, Raza MM, Kvedar JC. Health digital twins as tools for precision medicine: considerations for computation, implementation, and regulation. NPJ Digit Med. 2022;5:150.
14. Sun T, He X, Li Z. Digital twin in healthcare: recent updates and challenges. Digit Health. 2023;9:20552076221149651.
15. Shen S, Qi W, Liu X, et al. From virtual to reality: innovative practices of digital twins in tumor therapy. J Transl Med. 2025;23:348.
16. Gkintoni E, Halkiopoulos C. Digital twin cognition: AI-biomarker integration in biomimetic neuropsychology. Biomimetics. 2025;10:640.
17. Karakasis P, Antoniadis AP, Theofilis P, et al. Digital twin models in atrial fibrillation: charting the future of precision therapy? J Pers Med. 2025;15:256.
18. Olawade DB, Almarzook S, Ogunbona MA, Makanjuola BD, Olawuyi OF, Wada OZ. Digital twin applications in healthcare for people living with disability. Int J Med Inf. 2026;212:106359.
19. Bellman R. An introduction to artificial intelligence: can computers think? San Francisco: Boyd & Fraser Pub. Co.; 1978. Available from https://searchworks.stanford.edu/view/2762753 [accessed 26 June 2026].
21. Aung YYM, Wong DCS, Ting DSW. The promise of artificial intelligence: a review of the opportunities and challenges of artificial intelligence in healthcare. Br Med Bull. 2021;139:4-15.
22. Olawade DB, Wada OJ, David-olawade AC, Kunonga E, Abaire O, Ling J. Using artificial intelligence to improve public health: a narrative review. Front Public Health. 2023;11:1196397.
23. Sabanayagam C, Banu R, Lim C, et al. Artificial intelligence in chronic kidney disease management: a scoping review. Theranostics. 2025;15:4566-78.
24. Cho S, Kim H, Joh J. Digital twin and artificial intelligence technologies to assess the type IA endoleak. Bioengineering. 2025;13:1.
25. Mulder ST, Omidvari A, Rueten-budde AJ, et al. Dynamic digital twin: diagnosis, treatment, prediction, and prevention of disease during the life course. J Med Internet Res. 2022;24:e35675.
26. Jiang F, Jiang Y, Zhi H, et al. Artificial intelligence in healthcare: past, present and future. Stroke Vasc Neurol. 2017;2:230-43.
27. Li H, Zhang J, Zhang N, Zhu B. Advancing emergency care with digital twins. JMIR Aging. 2025;8:e71777.
28. Lee YK, Yoon E, Kim TH, Kim J, Kim J. Musculoskeletal digital therapeutics and digital health rehabilitation: a global paradigm shift in orthopedic care. J Clin Med. 2025;14:8467.
29. Shen M, Chen S, Ding X. The effectiveness of digital twins in promoting precision health across the entire population: a systematic review. NPJ Digit Med. 2024;7:145.
30. Prunella M, Altini N, D’alessandro R, et al. Pharmacometric and Digital Twin modeling for adaptive scheduling of combination therapy in advanced gastric cancer. Comput Methods Programs Biomed. 2025;270:108919.
31. Lei Z, Zhou H, Dai X, Hu W, Liu G. Digital twin based monitoring and control for DC-DC converters. Nat Commun. 2023;14:5604.
32. Guo Y, Liu Y, Sun W, et al. Digital twin-driven dynamic monitoring system of the upper limb force. Comput Methods Biomech Biomed Engin. 2023;27:1691-703.
33. Dihan MS, Akash AI, Tasneem Z, et al. Digital twin: data exploration, architecture, implementation and future. Heliyon. 2024;10:e26503.
34. Thangaraj PM, Benson SH, Oikonomou EK, Asselbergs FW, Khera R. Cardiovascular care with digital twin technology in the era of generative artificial intelligence. Eur Heart J. 2024;45:4808-21.
35. Avanzato R, Beritelli F, Lombardo A, Ricci C. Lung-DT: an AI-powered digital twin framework for thoracic health monitoring and diagnosis. Sensors. 2024;24:958.
36. Andres A, Roland M, Wickert K, et al. Advantages of digital twin technology in orthopedic trauma surgery - exploring different clinical use cases. Sci Rep. 2025;15:19987.
38. Hashimoto DA, Witkowski E, Gao L, Meireles O, Rosman G. Artificial intelligence in anesthesiology: current techniques, clinical applications, and limitations. Anesthesiology. 2020;132:379-94.
39. Saratkar SY, Langote M, Kumar P, Gote P, Weerarathna IN, Mishra GV. Digital twin for personalized medicine development. Front Digit Health. 2025;7:1583466.
40. Bordukova M, Makarov N, Rodriguez-esteban R, Schmich F, Menden MP. Generative artificial intelligence empowers digital twins in drug discovery and clinical trials. Expert Opin Drug Discov. 2023;19:33-42.
41. Meijer C, Uh H, El Bouhaddani S. Digital twins in healthcare: methodological challenges and opportunities. J Pers Med. 2023;13:1522.
42. Arksey H, O’malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19-32.
43. Levac D, Colquhoun H, O’brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69.
44. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467-73.
45. Guo Q, Jiang G, Zhao Q, et al. Rapid review: a review of methods and recommendations based on current evidence. J Evid Based Med. 2024;17:434-53.
46. Nørgaard B, Briel M, Chrysostomou S, et al. A systematic review of meta-research studies finds substantial methodological heterogeneity in citation analyses to monitor evidence-based research. J Clin Epidemiol. 2022;150:126-41.
47. Hernigou P, Olejnik R, Safar A, Martinov S, Hernigou J, Ferre B. Digital twins, artificial intelligence, and machine learning technology to identify a real personalized motion axis of the tibiotalar joint for robotics in total ankle arthroplasty. Int Orthop. 2021;45:2209-17.
48. Farhadiyadkuri F, Zhang X. A Five‐dimensional three‐layer digital twin to train a reinforcement learning agent for interaction control of a robotic exoskeleton in adolescent idiopathic scoliosis rehabilitation. Int J Mech Sys Dyn. 2025;5:385-400.
49. Hoyer G, Gao KT, Gassert FG, et al. Foundations of a knee joint digital twin from qMRI biomarkers for osteoarthritis and knee replacement. NPJ Digit Med. 2025;8:118.
50. Ahmadian H, Mageswaran P, Walter BA, et al. Toward an artificial intelligence‐assisted framework for reconstructing the digital twin of vertebra and predicting its fracture response. Int J Numer Method Biomed Eng. 2022;38:e3601.
51. Yu H, Huang Z, Liu Q, Carlucho I, Erden MS. Replication of impedance identification experiments on a reinforcement-learning-controlled digital twin of human elbows. In: 2024 International Joint Conference on Neural Networks (IJCNN); 2024 Jun 30-Jul 5; Yokohama, Japan. IEEE; 2024. pp. 1-8.
52. Jayakumar P, Rathouz PJ, Lin E, et al. Shared decision making using digital twins in knee osteoarthritis care: a randomized clinical trial of an AI-enabled decision aid versus education alone on decision quality, physical function, and user experience. eClinicalMedicine. 2025;89:103545.
53. Merzak L, Ott C, Saoutieff E, Gasnier P, Elhorga V, Boisseau S. Malalignment detection in TKA: a digital twin framework using instrumented tibial trays. IEEE Sens Lett. 2025;9:1-4.
54. Hernigou P, Safar A, Hernigou J, Ferre B. Subtalar axis determined by combining digital twins and artificial intelligence: influence of the orientation of this axis for hindfoot compensation of varus and valgus knees. Int Orthop. 2022;46:999-1007.
55. Stauffer T, Reber M, Fellmann L, Babst R, Meboldt M, Lohmeyer Q. Automated integration of surgical implants into digital twins for trauma surgery. In: Gee JC, Alexander DC, Hong J, Iglesias JE, Sudre CH, Venkataraman A, Golland P, Kim JH, Park J, Editors. Medical Image Computing and Computer Assisted Intervention - MICCAI 2025; 2025 Sep 23-27, Daejeon, South Korea. Cham: Springer; 2025. pp. 55-64.
56. Song X, He X, Li K, Lai X, Li Z. Construction method and application of human skeleton digital twin. Chin J Mech Eng. 2022;58:218-28. (in Chinese).
57. Wu H, Ji P, Ma H, Xing L. A comprehensive review of digital twin from the perspective of total process: data, models, networks and applications. Sensors. 2023;23:8306.
58. De Koning K, Broekhuijsen J, Kühn I, et al. Digital twins: dynamic model-data fusion for ecology. Trends Ecol Evol. 2023;38:916-26.
59. Saiz-vivó M, Mill J, Iriart X, et al. Digital twin integrating clinical, morphological and hemodynamic data to identify stroke risk factors. NPJ Digit Med. 2025;8:369.
60. Ren Y, Pieper AA, Cheng F. Utilization of precision medicine digital twins for drug discovery in Alzheimer’s disease. Neurotherapeutics. 2025;22:e00553.
61. Diniz P, Grimm B, Garcia F, et al. Digital twin systems for musculoskeletal applications: a current concepts review. Knee Surg Sports Traumatol Arthrosc. 2025;33:1892-910.
62. Laubenbacher R, Adler F, An G, et al. Toward mechanistic medical digital twins: some use cases in immunology. Front Digit Health. 2024;6:1349595.
63. Moser A, Appl C, Brüning S, Hass VC. Mechanistic mathematical models as a basis for digital twins. In: Herwig C, Pörtner R, Möller J, Editors. Digital Twins. Cham: Springer International Publishing; 2020. pp. 133-80.
64. Eminaga O, Abbas M, Kunder C, et al. Critical evaluation of artificial intelligence as a digital twin of pathologists for prostate cancer pathology. Sci Rep. 2024;14:5284.
65. Yao J, Yang Y, Wang X, Zhang X. Systematic review of digital twin technology and applications. Vis Comput Ind Biomed Art. 2023;6:10.
66. Ye X, Jamonnak S, Van Zandt S, Newman G, Suermann P. Developing campus digital twin using interactive visual analytics approach. Front Urban Rural Plan. 2024;2:9.
67. Vallée A. Digital twins for personalized medicine require epidemiological data and mathematical modeling: viewpoint. J Med Internet Res. 2025;27:e72411.
68. Rajaram A, Li H, Holodinsky JK, et al. Opening the black box: challenges and opportunities regarding interpretability of artificial intelligence in emergency medicine. CJEM. 2025;27:83-6.
69. Safavi S, Abdulnabi MSH, Rana ME, Alizadeh S. From black box to trustworthy AI: a secure framework for explainable cybersecurity decision-making. In: 2025 International Conference on Advancements in Smart, Secure and Intelligent Computing (ASSIC); 2025 May 16-18; Bhubaneswar, India. IEEE; 2025. pp. 1-4.
70. Ting DSW, Pasquale LR, Peng L, et al. Artificial intelligence and deep learning in ophthalmology. Br J Ophthalmol. 2019;103:167-75.
71. Laubenbacher R, Mehrad B, Shmulevich I, Trayanova N. Digital twins in medicine. Nat Comput Sci. 2024;4:184-91.
72. Lu R, She C, He D, et al. AI enhanced diagnostic accuracy and workload reduction in hepatocellular carcinoma screening. NPJ Digit Med. 2025;8:500.
73. Hong EK, Ham J, Roh B, et al. Diagnostic accuracy and clinical value of a domain-specific multimodal generative AI model for chest radiograph report generation. Radiology. 2025;314:e241476.
74. Ashrafi S, Ahmadieh H, Bayat K, et al. Diagnostic accuracy of AI models in detecting different inherited retinal diseases: a systematic review and meta-analysis. Trans Vis Sci Tech. 2025;14:22.
75. Zsidai B, Hilkert AS, Kaarre J, et al. ; ESSKA Artificial Intelligence Working Group. A practical guide to the implementation of AI in orthopaedic research - part 1: opportunities in clinical application and overcoming existing challenges. J Exp Orthop. 2023;10:117.
76. Tiwari RG, Vimal V, Agarwal AK. Opening the black box: explainable AI insights into obesity prediction using SMOTE-balanced stacking ensembles. In: 2024 IEEE 16th International Conference on Computational Intelligence and Communication Networks (CICN); 2024 Dec 22-23; Indore, India. IEEE; 2024. pp. 1127-31.
77. Tosun AB, Pullara F, Becich MJ, Taylor DL, Fine JL, Chennubhotla SC. Explainable AI (xAI) for anatomic pathology. Adv Anat Pathol. 2020;27:241-50.
78. Karim MR, Islam T, Shajalal M, et al. Explainable AI for bioinformatics: methods, tools and applications. Brief Bioinform. 2023;24:bbad236.
79. Sanjan S, Kumar GDP, Suraj P, Rohan UA, Srinivas R, Thanush V. Bridging the black box: interpreting transformer attention in high-stakes medical and legal AI. In: 2024 Third International Conference on Trends in Electrical, Electronics, and Computer Engineering (TEECCON); 2024 Nov 7-8; Bangalore, India. IEEE; 2024. pp. 35-40.
80. Liu JJ, Borsari B, Li Y, et al. Digital phenotyping from wearables using AI characterizes psychiatric disorders and identifies genetic associations. Cell. 2025;188:515-529.e15.
81. Famularo S, Boldrini L, Donadon M, Morise Z. Interpretable and OpenAI models: a mandate for the future of HCC diagnostics. Liver Int. 2025;45:e16229.
82. Wen B, Wu Y, Daqqaq T, Chaddad A. Towards a transparent and interpretable AI model for medical image classifications. Cogn Neurodyn. 2025;19:149.
83. Hiraoka A, Swinnen B, Vandeputte A, Franssen W, Leirs G. Optimizing operating room efficiency in robotic‐assisted total knee arthroplasty through manufacturing efficiency principles. J Exp Orthop. 2025;12:e70283.
84. Albertini J, Derycke L, Millon A, Soler R. Digital twin and artificial intelligence technologies for predictive planning of endovascular procedures. Semin Vasc Surg. 2024;37:306-13.
85. Kludt C, Wang Y, Ahmad W, et al. Next-generation lung cancer pathology: development and validation of diagnostic and prognostic algorithms. Cell Rep Med. 2024;5:101697.
86. Misir A, Yuce A. AI in orthopedic research: a comprehensive review. J Orthop Res. 2025;43:1508-27.
87. Shu H, Liang R, Li Z, et al. Twin-S: a digital twin for skull base surgery. Int J Comput Assist Radiol Surg. 2023;18:1077-84.
88. Silfvergren O, Simonsson C, Ekstedt M, Lundberg P, Gennemark P, Cedersund G. Digital twin predicting diet response before and after long-term fasting. PLoS Comput Biol. 2022;18:e1010469.
89. Rowan NJ. Digital technologies to unlock safe and sustainable opportunities for medical device and healthcare sectors with a focus on the combined use of digital twin and extended reality applications: a review. Sci Total Environ. 2024;926:171672.
90. Mo D, Tien C, Yeh Y, et al. Design of digital-twin human-machine interface sensor with intelligent finger gesture recognition. Sensors. 2023;23:3509.
91. Seth I, Lim B, Lu PYJ, et al. Digital twins use in plastic surgery: a systematic review. J Clin Med. 2024;13:7861.
92. Asciak L, Kyeremeh J, Luo X, et al. Digital twin assisted surgery, concept, opportunities, and challenges. NPJ Digit Med. 2025;8:32.
93. Tang X, Wang D, Mou P, et al. Addition of infiltration between the popliteal artery and the capsule of the posterior knee (IPACK) to local infiltration analgesia for total knee arthroplasty: a prospective randomized controlled trial. J Arthroplasty. 2023;38:1484-92.
94. Tang X, Yang Y, Zheng F, Ma L, Li P. A commentary on ‘Duloxetine for rehabilitation after total knee arthroplasty: a systematic review and meta-analysis’. Int J Surg. 2023;109:3683-6.
95. Wang W, Li J, Liu L, et al. Role of circular RNA expression in the pathological progression after spinal cord injury. Neural Regen Res. 2021;16:2048-55.
96. Xiang L, Gu Y, Deng K, et al. Integrating personalized shape prediction, biomechanical modeling, and wearables for bone stress prediction in runners. NPJ Digit Med. 2025;8:276.
97. Skalidis I, Maurizi N, Salihu A, et al. Artificial intelligence and advanced digital health for hypertension: evolving tools for precision cardiovascular care. Medicina. 2025;61:1597.
98. Magyar P, Hegedűs-kuti J, Szőlősi J, Farkas G. Real-time data visualization of welding robot data and preparation for future of digital twin system. Sci Rep. 2024;14:10229.
99. He W, Wu X, Jin Z, et al. Generative artificial intelligence in medical imaging: current landscape, challenges, and future directions. Interdiscip Med. 2025;3:e20250024.
100. Cong S, Wang H, Zhou Y, Wang Z, Yao X, Yang C. Comprehensive review of Transformer‐based models in neuroscience, neurology, and psychiatry. Brain-X. 2024;2:e57.
101. Bofill J, Abisado M, Villaverde J, Sampedro GA. Exploring digital twin-based fault monitoring: challenges and opportunities. Sensors. 2023;23:7087.
102. Javed AR, Khan HU, Alomari MKB, et al. Toward explainable AI-empowered cognitive health assessment. Front Public Health. 2023;11:1024195.
103. Ghassemi M, Oakden-rayner L, Beam AL. The false hope of current approaches to explainable artificial intelligence in health care. Lancet Digit Health. 2021;3:e745-50.
104. Van Der Velden BH, Kuijf HJ, Gilhuijs KG, Viergever MA. Explainable artificial intelligence (XAI) in deep learning-based medical image analysis. Med Image Anal. 2022;79:102470.
105. Gunning D, Stefik M, Choi J, Miller T, Stumpf S, Yang G. XAI-explainable artificial intelligence. Sci Robot. 2019;4:eaay7120.
106. Räz T, Pahud De Mortanges A, Reyes M. Explainable AI in medicine: challenges of integrating XAI into the future clinical routine. Front Radiol. 2025;5:1627169.
107. Hernigou P, Scarlat MM. Ankle and foot surgery: from arthrodesis to arthroplasty, three dimensional printing, sensors, artificial intelligence, machine learning technology, digital twins, and cell therapy. Int Orthop. 2021;45:2173-6.
108. Leal MOC, Díaz DM, Romo CO, et al. Biomechanics digital twin: markerless joint acceleration prediction using machine learning and computer vision. In: 2023 Future of Educational Innovation-Workshop Series Data in Action: Digital Ecosystem and Emerging Tools for Education; 2023 Jan 16-18; Monterrey, Mexico. IEEE; 2023. pp. 1-8.
109. Wang W, Su Y, Tang S, et al. Identification of noncoding RNA expression profiles and regulatory interaction networks following traumatic spinal cord injury by sequence analysis. Aging. 2019;11:2352-68.
110. Wang W, Liu C, He D, et al. CircRNA CDR1as affects functional repair after spinal cord injury and regulates fibrosis through the SMAD pathway. Pharmacol Res. 2024;204:107189.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.