


Pediatric mesenteric lymphangioma leading to extensive small bowel torsion and transplant rescue: a case report
 0
0 Abstract
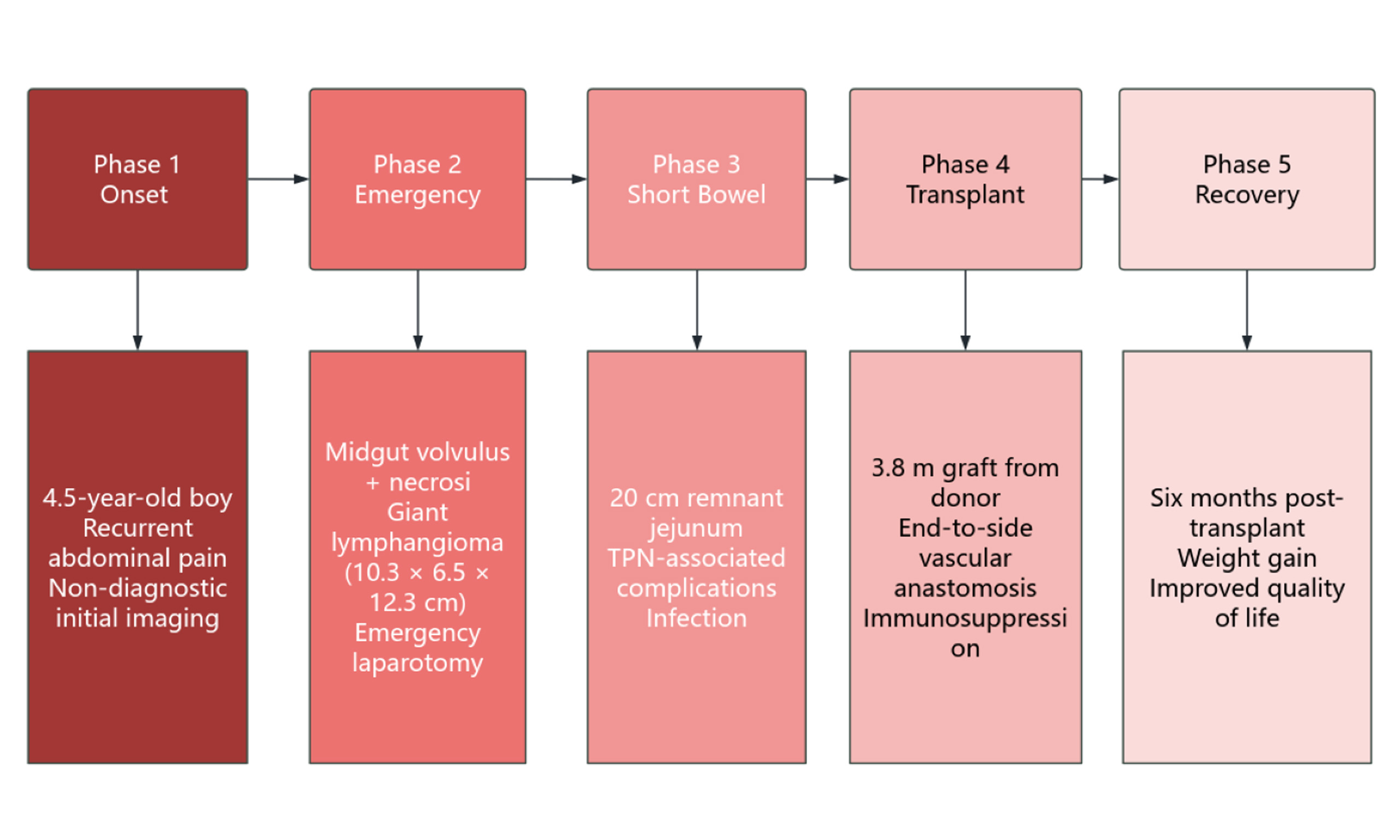
We report the case of a 4.5-year-old boy with recurrent abdominal pain caused by a giant mesenteric lymphangioma, which led to severe midgut volvulus, ischemic necrosis, and ultra-short bowel syndrome (remnant small bowel length: 20 cm). After emergency resection, he developed short bowel syndrome with life-threatening complications, including cholestatic liver injury, catheter‑related bloodstream infection, and severe hypokalemia with convulsions. He ultimately underwent successful small bowel transplantation, was discharged on postoperative day 48, and showed improved nutritional status at six months postoperatively. This case highlights that mesenteric lymphangioma, although benign, can cause bowel volvulus requiring transplantation; prompt advanced imaging for recurrent pediatric abdominal pain is crucial; and small bowel transplantation is a definitive therapy for irreversible intestinal failure with total parenteral nutrition (TPN) complications.
Keywords
INTRODUCTION
Mesenteric lymphangioma is a benign neoplasm originating from hyperplastic, thin-walled lymphatic channels. Approximately 70% arise in the head and neck region, 20% in the axillary region, and only 10% involve the greater momentum, colonic mesentery, or retroperitoneal space[1,2]. The exact etiology of mesenteric lymphangioma remains unclear, but it is generally believed to result from abnormal development of the lymphatic system during embryonic development. In some cases, it may be associated with genetic factors or other congenital conditions. Nevertheless, most cases have no family history or genetic predisposition[3]. These lesions primarily occur in the mesentery but may also extend to adjacent structures. Although most lesions are asymptomatic, this lesion may give rise to complications such as torsion, hemorrhage, and rupture. These sequelae can trigger an acute abdomen, thereby necessitating emergent surgical intervention[4]. Ischemic necrosis secondary to midgut volvulus caused by a mesenteric lymphangioma represents an extremely rare and severe complication, with limited studies available. Short bowel syndrome presents a major therapeutic challenge, and small bowel transplantation remains the definitive treatment to achieve independence from parenteral nutrition and improve quality of life in affected patients.
METHODS
This case report was conducted in accordance with the CARE (CAse Report) guidelines. All procedures involving human participants were reviewed and approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology {approval number: [2024] LunShenZi (0040-01)}. Written informed consent to participate in this case report was obtained from the patient’s legal guardians. All clinical data and images were anonymized, and no information that could identify the patient is included in this article.
CASE PRESENTATION
Patient information and present illness
A 4.5-year-old boy initially presented on April 9, 2024, with abdominal pain. Ultrasonography revealed gas-filled, dilated bowel loops. His clinical condition improved after symptomatic management. On April 29, abdominal pain recurred and was accompanied by vomiting, and conservative management proved ineffective. The patient was transferred to the Children’s Hospital on May 2 with diagnoses of sepsis and bowel obstruction and was admitted to the intensive care unit (ICU). Exploratory laparotomy on May 3 revealed a massive mesenteric lymphangioma (approximately 10.3 × 6.5 × 12.3 cm) that had caused small bowel torsion with resultant ischemic necrosis. Consequently, the majority of the small intestine along with the ileocecal region was resected, and an end-jejunostomy was created from the approximately 20 cm of remaining viable jejunum. Postoperatively, antimicrobial therapy and nutritional support were administered. However, the patient’s nutritional status progressively deteriorated, developing jaundice and liver dysfunction. On June 10, a wound infection complicated the clinical course, necessitating incision and drainage. A cloudy, pale-yellow exudate was noted around the stoma site.
Admission physical examination
The patient had mild jaundice. Subcutaneous fat was decreased in the limbs and abdominal wall. The abdomen was scaphoid and soft. A stoma was visible in the left abdomen with ulcerated peristomal skin. A pinpoint fistulous tract was noted near the umbilicus. An old surgical incision approximately 7 cm long was visible below the umbilicus, with a subcutaneous drain in its center, draining turbid yellow fluid.
Timeline
The patient’s clinical course was complex and critical, from initial onset through emergency surgery and small bowel transplantation to six months postoperatively. To illustrate the disease progression, key interventions, and major clinical events in chronological order, a detailed timeline is summarized in Table 1.
Case timeline from initial presentation to six months postoperatively
| Date/Time point | Key clinical events | Interventions |
| April 9, 2024 | A 4.5-year-old boy initially presented with abdominal pain | Ultrasonography showed gas-filled, dilated bowel loops; symptomatic management led to improvement |
| April 29, 2024 | Abdominal pain recurred with vomiting; conservative management failed | - |
| May 2, 2024 | Diagnosed with sepsis and bowel obstruction | Transferred to the Children’s Hospital and admitted to the ICU |
| May 3, 2024 | Emergency laparotomy revealed a giant mesenteric lymphangioma causing small bowel torsion and ischemic necrosis | Massive small bowel resection (only 20 cm of jejunum remained) with end-jejunostomy |
| Post-resection (after May 3, 2024) | Progressive deterioration of nutritional status; jaundice and impaired liver function developed | Antimicrobial therapy; nutritional support |
| June 10, 2024 | Wound infection; cloudy, pale-yellow exudate noted around the stoma site | Incision and drainage |
| Post-resection day 15 (approx. May 18, 2024) | Unexplained high-grade fever (peak 40 °C) without abdominal distension or pain | Empirical cefoperazone; after peripherally inserted central catheter (PICC) removal, tip culture confirmed Gram-negative bacilli, switched to meropenem |
| Transitional period (short bowel syndrome management) | Severe hypokalemia (2.38 mmol/L) precipitating convulsions; hypoglycemia (1.9 mmol/L) | Nutritional optimization by a nutritionist; multidisciplinary team assessment; listed for small bowel transplantation |
| Day of transplantation | Received a 3.8-meter small bowel graft from a brain-dead donor | Bowel continuity restored; diverting T-loop stoma created |
| Postoperative day 15 (POD 15) | Enteral nutrition initiated and well tolerated | Gradual advancement of enteral feeds |
| Postoperative day 18 (POD 18) | Satisfactory wound healing | Sutures removed |
| Postoperative day 20 (POD 20) | High stoma output; transient hyperkalemia | Switched to formula pump feeding; renal function monitored |
| Postoperative day 26 (POD 26) | Condition stabilized | Transferred from the ICU to surgical ward |
| Postoperative day 48 (POD 48) | Stable condition | Discharged |
| Six months postoperatively | Weight gain, improved nutritional status, markedly enhanced quality of life | Serum tacrolimus concentration monitored; surveillance colonoscopy biopsy showed no definite acute rejection |
Investigations
Preoperative imaging (before small bowel transplantation)
Abdominal aortic computed tomography angiography (CTA) and plain computed tomography (CT) scans of the upper and lower abdomen revealed: status post partial small bowel resection with jejunostomy and a mildly thickened and edematous gallbladder wall suggestive of cholecystitis. CTA demonstrated irregular narrowing of the superior mesenteric artery lumen with a cystic protrusion on the right side distally, suggesting either vasculitis with tumor-like dilatation or postoperative changes [Figure 1].
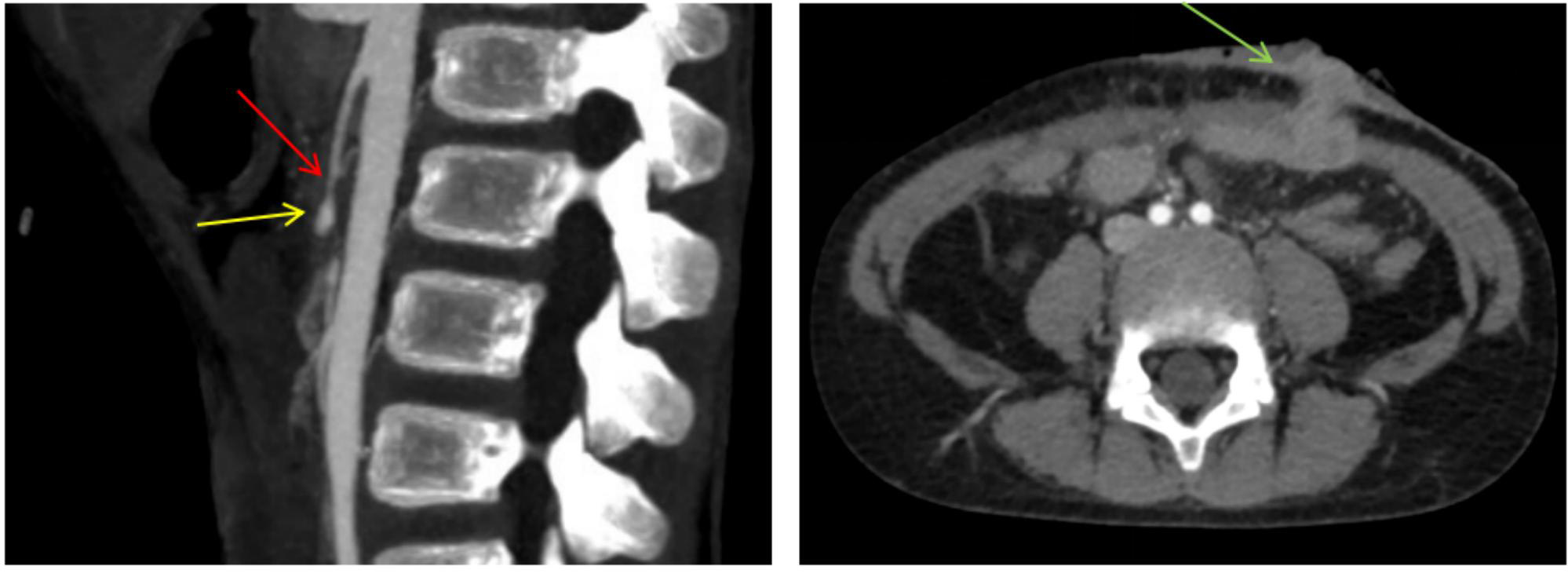
Figure 1. Preoperative CTA scan and CT showing the mesenteric lesion and post-jejunostomy changes. Left: Sagittal view showing the superior mesenteric artery trunk with luminal narrowing (red arrow) and a distal cystic protrusion (yellow arrow). Right: Axial view showing anterior abdominal wall post-jejunostomy changes (green arrow). CTA: Computed tomography angiography; CT: computed tomography.
Preoperative pathology (before small bowel transplantation)
Mesenteric lymphangioma (macrocystic type) of the jejunal mesentery. Secondary to bowel volvulus, hemorrhagic infarction of the small bowel and ileocecal segment was noted. Hemorrhagic infarction of the appendix. Hemorrhage and necrosis were identified at both surgical resection margins.
Preliminary diagnoses
Short bowel syndrome; cholestatic hepatitis; severe malnutrition with cachexia; status post jejunostomy; abdominal wall infectious sinus tract; status post small bowel resection.
Management course
• Phase One: Control of Intra-Abdominal Infection
A comprehensive CT scan was performed after admission to exclude lymphangiomas at other sites.
Surgical record: The original surgical incision was debrided, and purulent fluid was evacuated. A purulent sinus tract, indicative of an intra-abdominal abscess with an abdominal wall fistula, was identified. The incision was extended to access the abdomen, followed by debridement of the abscess and copious irrigation. A single abdominal drain was placed and secured. After achieving hemostasis and closing the abdomen, the abdominal wall wound was irrigated, debrided, and sutured. A 16-gauge neurosurgical drain was also secured at the stoma site.
• Phase Two: Transitional Management for Short Bowel Syndrome
The patient was transferred to the general ward postoperatively with continuous monitoring of vital signs. On postoperative day 15, he developed an unexplained high-grade fever (peak 40 °C) without abdominal distension, pain, or other discomfort. The stoma was well-perfused, with yellow, loose stools in the stoma bag. Physical examination and abdominal ultrasound were unremarkable. The patient had recurrent fever episodes accompanied by profuse sweating, requiring increased fluid resuscitation. Elevated inflammatory markers led to empirical cefoperazone administration, which reduced the fever. Clinical evaluation identified no pulmonary or abdominal source of infection. Potential sources included prolonged use of a peripherally inserted central catheter (PICC), extended high-concentration parenteral nutrition, and a history of repeated thrombolysis. Following PICC removal, tip culture revealed Gram-negative bacilli, prompting initiation of meropenem (20 mg/kg every 8 h) and subsequent clinical improvement. A nutritionist was consulted for nutritional optimization.
• Phase Three: Small Bowel Transplantation
(1) Indications for Transplant Assessment: During the transitional period, the patient developed severe hypokalemia (serum potassium 2.38 mmol/L) with convulsions, and hypoglycemia (fasting blood glucose
(2) Surgical Record: The graft, a 3.8-meter small bowel segment from a brain-dead donor, was allocated through the China Organ Transplant Resource Sharing Computerized System (COTRS) and procured under standard protocols with ethical committee approval. At laparotomy, severe intra‑abdominal adhesions were encountered. The native small intestine remnant measured approximately 20 cm distal to the Treitz ligament. After extensive adhesiolysis, the left upper quadrant stoma was taken down. The donor’s vascular pedicles were trimmed, with bleeding branches ligated, and the graft was flushed and stored in ice-cold preservation solution (cold ischemia time: 90 min). The recipient’s infrarenal aorta and inferior vena cava were exposed. Vascular anastomoses were performed in an end-to-side fashion: first, the donor superior mesenteric artery (SMA) to the recipient aorta, followed by the donor superior mesenteric vein (SMV) to the recipient inferior vena cava (IVC), using a two-stitch technique for each anastomosis (warm ischemia time: 10 min). Upon reperfusion, the graft regained a healthy color and peristalsis after rehydration with warm saline. Bowel continuity was restored with a hand-sewn overlapping anastomosis between the native distal bowel and the donor proximal jejunum, and a second similar anastomosis to the transverse colon stump, both reinforced with seromuscular sutures. A diverting T-loop stoma was created in the right lower quadrant. A three-lumen gastrostomy tube was placed in the left upper abdomen. The abdomen was closed in layers over three drainage tubes.
Postoperative management
The patient was transferred to the ICU for close monitoring and specialist care.
(1) Supportive and symptomatic management was provided, with careful control of vital signs, including blood pressure, temperature, and heart rate.
(2) Antimicrobial therapy comprised cefoperazone, ganciclovir, and voriconazole, supplemented with vancomycin.
(3) An intensive immunosuppression regimen was implemented, including azathioprine and tacrolimus (with concentration monitoring), supplemented with high-dose methylprednisolone pulse therapy.
(4) Enhanced supportive care and nutritional management were provided, including parenteral nutrition support, monitoring of electrolyte balance, and prompt correction of electrolyte imbalances.
(5) The color, output volume, and consistency of the transplanted bowel stoma were closely monitored. Surveillance colonoscopies showed healthy graft mucosa.
(6) Hepatic and renal function were monitored; hepatoprotective and choleretic agents such as glutathione and deoxycholic acid were administered.
Postoperative recovery
Enteral nutrition was initiated on postoperative day (POD) 15 and was well tolerated. Sutures were removed on POD 18. Due to high stoma output, a nutrition consultation on POD 20 resulted in a switch to formula pump feeding, which improved absorption and allowed gradual advancement of enteral feeds. Transient fluid imbalance with hyperkalemia on POD 20 raised concern for renal impairment, but the patient’s condition stabilized by POD 26. With enteral nutrition successfully advanced without any signs of intolerance, the patient was transferred from the ICU to the surgical ward and was discharged in stable condition on POD 48.
Postoperative examination
Postoperative imaging
Postoperative CT imaging showed the transplanted small bowel graft [Figure 2]. No significant abnormalities of the transplanted graft or surrounding structures were observed.

Figure 2. Postoperative CT scan following small bowel transplantation showed no significant abnormalities involving the transplanted graft or adjacent structures. CT: Computed tomography.
Pathological findings
The post-transplantation endoscopic biopsy specimen showed an intact mucosal epithelial layer and regularly arranged glands within the lamina propria. Minimal scattered lymphocytes and plasma cells infiltrated the interstitial stroma. Occasional apoptotic bodies were noted in the crypts (1-3 per 10 crypts). Acute rejection grading: suspected or indeterminate acute rejection.
FOLLOW UP
At six months after transplantation, the patient exhibited weight gain and improved nutritional status, with markedly enhanced quality of life according to clinical assessment and guardian reports. Histopathology revealed preserved villous architecture in the small intestine with scattered chronic inflammatory cell infiltration within the lamina propria. The patient adhered well to the immunosuppressive regimen (tacrolimus and azathioprine) as evidenced by regular therapeutic drug monitoring and guardian medication logs, and enteral nutrition was well tolerated with successful advancement to full feeds by discharge. No adverse or unanticipated events were reported during the six months after transplantation.
DISCUSSION
Mesenteric lymphangiomas are benign lesions that rarely occur in the abdomen, accounting for approximately 5% of all lymphangiomas[3]. Small bowel mesenteric lymphangiomas are particularly rare[5], yet they represent a potentially fatal cause of acute bowel obstruction or volvulus[6]. As illustrated by this case, the nonspecific symptoms prior to an acute abdomen make preoperative diagnosis difficult; initial imaging may show only dilated bowel loops, leading to delays in diagnosis and treatment[7]. Therefore, mesenteric masses should be considered in children with recurrent abdominal pain, and early contrast-enhanced CT or magnetic resonance imaging (MRI) is crucial for timely diagnosis[8].
Thapa et al.[2] described a pediatric case of volvulus without resultant ultra-short bowel syndrome. In contrast, our patient’s giant mesenteric lymphangioma (10.3 × 6.5 × 12.3 cm) led to catastrophic torsion, leaving only 20 cm of viable jejunum - one of the shortest residual lengths reported after mesenteric lymphangioma-induced volvulus, placing the patient at the extreme end of the short bowel syndrome spectrum. Furthermore, Moulin et al.[9] reported that intestinal failure requiring transplantation secondary to a mesenteric lymphangioma is exceedingly rare, highlighting the rarity of our case.
Ultra-short bowel syndrome following massive resection for mesenteric lymphangioma has only been sporadically reported in the literature[3]. The patient’s clinical decline confirmed the presence of irreversible intestinal failure, making small bowel transplantation the definitive therapy per international criteria[10]. Our patient achieved graft survival and enteral autonomy at six months, consistent with the reported 1-year graft survival of 75%-85% in pediatric transplantation[11], and nutritional recovery aligned with typical enteral autonomy within 2-4 weeks post-transplant[12].
This case offers three key lessons. First, mesenteric lymphangiomas, though benign, can precipitate volvulus requiring resection; clinicians should maintain a high suspicion for mesenteric masses in children with unexplained recurrent abdominal pain and obtain prompt advanced imaging. Second, for children with short bowel syndrome and life-threatening TPN complications, small bowel transplantation is a definitive and life-saving therapy. Third, multidisciplinary team collaboration - from intensive care to transplant surveillance - is essential for optimizing outcomes.
PATIENT PERSPECTIVE
The patient’s mother recalled: “When my son first had abdominal pain, we thought it was nothing serious. Even after the first hospital visit, no clear cause was found. When his condition suddenly worsened and required emergency surgery, we were devastated to learn that most of his small bowel had to be removed, leaving only 20 cm. The following months were very difficult. The small bowel transplant gave him a second chance. Now, six months after the transplant, he can eat, gain weight, and live a normal life again. We hope other families can learn from our experience”.
CONCLUSION
This case demonstrates that mesenteric lymphangiomas, despite their benign histology, can precipitate catastrophic midgut volvulus necessitating small bowel transplantation. A more thorough initial evaluation upon presentation may have altered the clinical course. For children who develop short bowel syndrome with life-threatening TPN complications, transplantation remains the definitive therapy to restore bowel function and quality of life. We therefore advocate for early referral of patients with complex mesenteric lymphangiomas to specialized transplant centers. Specifically, referral should be initiated without delay, ideally within 2-4 weeks after bowel resection, when residual small bowel is less than 30 cm, or when TPN-related complications (e.g., cholestatic liver injury, recurrent catheter-related sepsis, severe electrolyte disturbances) emerge. Furthermore, intestinal rehabilitation programs should be considered as a bridge to transplantation. These multidisciplinary programs may help maximize enteral absorption and potentially delay or even prevent transplantation in some cases. However, when irreversible intestinal failure is evident, as in our patient, transplant evaluation and listing should proceed concurrently with rehabilitation. A multidisciplinary approach from diagnosis through long-term follow-up is therefore essential for optimizing outcomes.
DECLARATIONS
Authors’ contributions
Searched and collected related articles and drafted the manuscript: Cheng F
Assisted with data collection and validation: Huang Y, Liu X
Conceived the topic, revised the manuscript and secured funding for publication: Wu K
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This research was funded by the National Natural Science Foundation of China (No. 82273302) and the General Project of Hubei Natural Science Foundation (No. 2020CFB766).
Conflicts of interest
Wu K is an Editorial Board Member of Rare Disease and Orphan Drugs Journal. Wu K was not involved in any steps of editorial processing, notably including reviewers’ selection, manuscript handling and decision making. The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
This study involving a human participant was reviewed and approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology {approval number: [2024] LunShenZi (0040-01)}. Written informed consent to participate in this case report was obtained from the patient’s legal guardians.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Mojahid A, Benramdane H, Mahi NE, et al. Small bowel volvulus induced by cystic lymphangioma in a 12-year-old child: case report. Radiol Case Rep. 2025;20:4381-4.
2. Thapa S, Sharma A, Upreti D, et al. A huge mesenteric lymphangioma presenting as a small bowel volvulus in a paediatric patient: a case report. Case Rep Pathol. 2022;2022:3033705.
3. Shaker K, Alomar K, Dawarah M, Brnbow Z, Alnwaijie N, Khouri L. A rare case of a large mesenteric lymphangioma in a 2-year-old child: case report and review of the literature. Int J Surg Case Rep. 2024;116:109409.
4. Mhand M, Rhoul C, Bouhout T, Serji B. Cystic lymphangioma of the mesentery in an adult: a case report and literature review. Cureus. 2024;16:e63412.
5. Suthiwartnarueput W, Kiatipunsodsai S, Kwankua A, Chaumrattanakul U. Lymphangioma of the small bowel mesentery: a case report and review of the literature. World J Gastroenterol. 2012;18:6328-32.
6. Chang TS, Ricketts R, Abramowsky CR, et al. Mesenteric cystic masses: a series of 21 pediatric cases and review of the literature. Fetal Pediatr Pathol. 2011;30:40-4.
7. Barbu LA, Mărgăritescu ND, Cercelaru L, et al. Mesenteric cysts as rare causes of acute abdominal masses: diagnostic challenges and surgical insights from a literature review. J Clin Med. 2025;14:4888.
8. Ajmera P, Jadhav V. Painful abdominal lump in the pediatric age group: a diagnostic dilemma. Cureus. 2021;13:e13202.
9. Moulin L, Rumbo C, Romero P, et al. Case report: multivisceral transplantation for an extensive cystic lymphangioma of the mesenteric root. Transplant Proc. 2016;48:543-5.
10. Raghu VK, Rumbo C, Horslen SP. From intestinal failure to transplantation: review on the current need for transplant indications under multidisciplinary transplant programs worldwide. Pediatr Transplant. 2024;28:e14756.
11. Amin A, Farmer DG. Current outcomes after pediatric and adult intestinal transplantation. Curr Opin Organ Transplant. 2019;24:193-8.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.