
Advances in sudden unexplained death: novel insights into technical innovations and their applications in forensic investigation
 0
0 Abstract
Sudden unexplained death (SUD) remains a major challenge in forensic practice, as conventional autopsy and systemic histological examination often fails to identify a definitive cause. Up to 10%-15% of cases are classified as SUD, underscoring the need for advanced technical innovations. This review aims to summarize recent advances in the forensic investigation of SUD, focusing on technical innovations, including molecular autopsy, multi-omics approaches, virtual autopsy techniques, and the application of artificial intelligence (AI). In brief, molecular autopsy has evolved from Sanger sequencing to next-generation sequencing (NGS) technologies, enabling high-throughput screening of genes associated with SUD due to channelopathies and cardiomyopathies, in which multiple pathogenic/likely pathogenic variants in major causative genes such as SCN5A, KCNQ1, and KCNH2 have been identified. Multi-omics strategies including proteomics, metabolomics, transcriptomics, and spectroscopic techniques such as Raman spectroscopy and Fourier transform infrared (FTIR) spectroscopy, provide functional insights into premortem biochemical states and can detect subtle molecular abnormalities that are valuable in identifying SUD. In addition, virtual autopsy techniques, including postmortem CT, CT angiography and MRI, offer non-invasive detection of subtle abnormalities and guide targeted sampling. By enhancing the interpretation of genetic variants, omics data, and imaging patterns, AI facilitates the identification of causes of death in SUDs. Despite rapid progress in this area, such techniques have not yet been integrated into routine postmortem diagnostic criteria in forensic medicine. Further research and standardization are needed to integrate these methods into forensic practice and disease prevention, thereby clarifying disease mechanisms and helping prevent additional fatalities in affected families.
Keywords
INTRODUCTION
Sudden unexplained death syndrome (SUDS), first proposed in 1917 in Philippines, describes deaths for which no apparent clinical cause can be identified, typically in cases where an autopsy has not been performed[1]. In 2003, the concept of sudden arrhythmic death syndrome (SADS) was introduced in clinical practice, replacing the earlier term "sudden adult death syndrome". The definition of SADS attributes all unexplained deaths to cardiac causes, i.e., sudden cardiac death (SCD). SADS refers to cases in which death remains unexplained following a comprehensive postmortem examination, including histological and toxicological analysis[2,3], comparable to sudden infant death syndrome (SIDS), a diagnosis of unexplained death in infant. Cardiac electrophysiological disorders are considered the leading cause in such cases, where death is attributed to electrical dysfunction in the absence of structural heart disease[2]. As one of the major health problems in the world, SCD accounts for approximately 50% of all cardiovascular deaths[4], and is the main cause of death (COD) for 43.9% of sudden death cases based on forensic autopsy[5]. The annual incidence of SCD is 41.8/100,000 persons in China[6], with about 0.001% in adolescents and young adults (< 35 years), 0.1% in the subjects between 35 to 40 years, 0.2% by 60 years, increasing to 20% in the elderly population[7]. The prevalence of SADS ranges from 4% to 53% in European countries[8], ~ 35% in deaths of young adult males aged 18 ~ 35 years in the US[9], while the data in China remains absent.
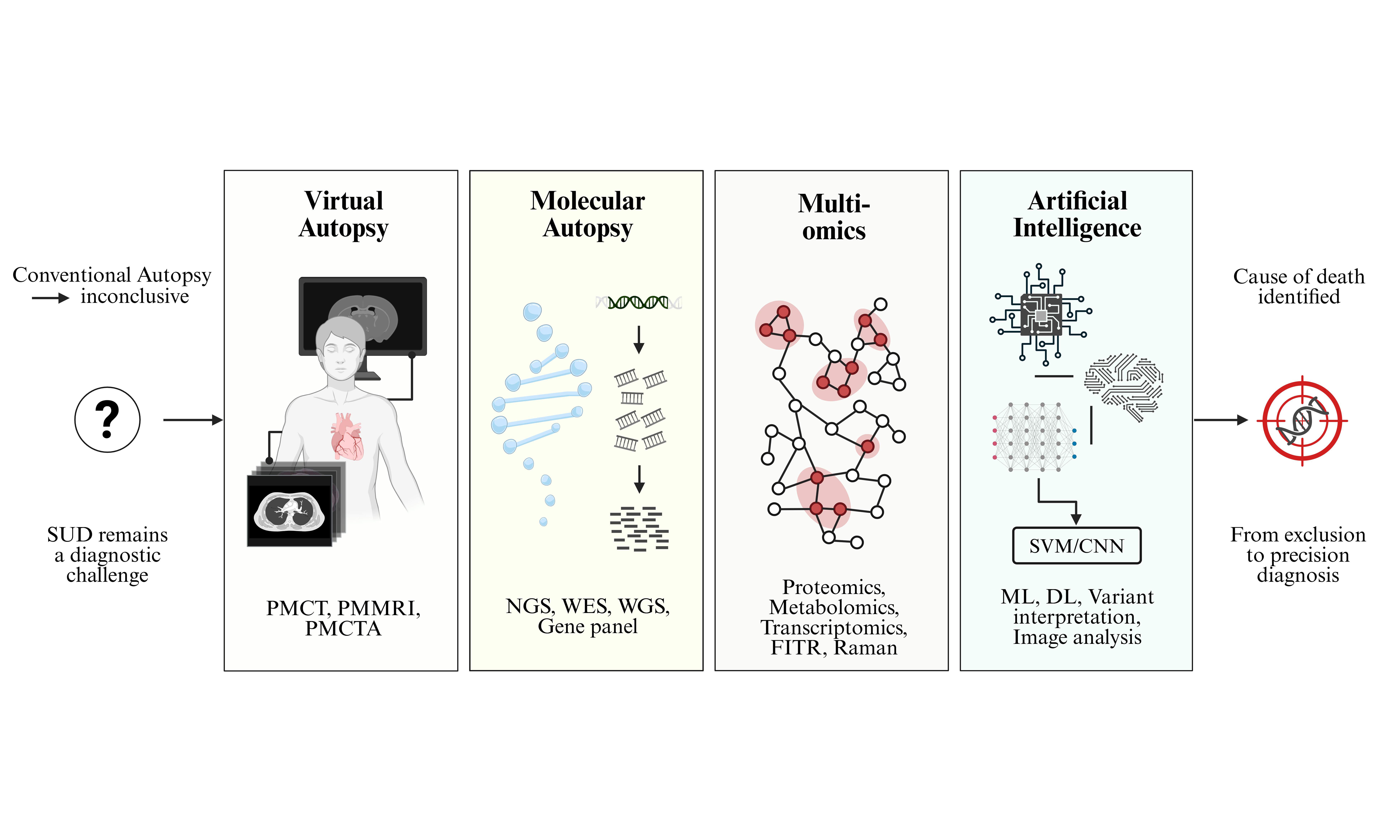
In forensic practice, a death is classified as unascertained only by exclusion - that is, when autopsy and toxicological investigations yield inconclusive results, the heart is structurally normal on both gross and histological examination, and all non-cardiac etiologies have been ruled out[7]. These unexplained sudden deaths occurring in an individual older than 1 year are defined as sudden unexplained deaths (SUDs)[10]. In previous studies, approximately one-half of the sudden unexpected deaths had specific findings at autopsy, supporting a non-arrhythmic mechanism for the sudden death, such as acute myocardial infarction (AMI), cardiac rupture, acute heart failure (HF), and acute pulmonary embolus; while the other one-half of the sudden deaths, resulting from arrhythmia or non-cardiac etiologies such as epilepsy and electrolyte disturbance, had no specific findings at autopsy and follow-up histopathological examination[11,12]. The incidence of unascertained deaths varies depending on several factors, including out-of-hospital deaths lacking clinical records, postmortem decomposition that compromises pathological or toxicological evidence, the completeness of the initial autopsy, the thoroughness of ancillary investigations, and the experience of the pathologist[13]. For example, COD of SCDs caused by abnormal electrophysiology can be hardly recognized after death if the medical history and electrocardiography (ECG) are absent. Figure 1 illustrates the hierarchical and overlapping relationships among the key entities of sudden death: SIDS (age < 1 year), SUD (age ≥ 1 year, autopsy-negative), SCD (all cardiac causes), SADS (arrhythmic subset of SUD), and SUDEP (sudden death in epilepsy, which may overlap with SADS).
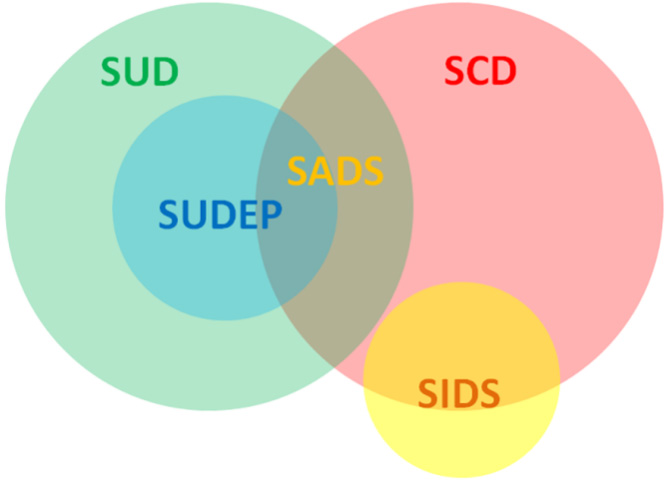
Figure 1. Venn diagram illustrating the relationships among SUD, SCD, SADS, SUDEP, and SIDS. The diagram highlights the age-based distinction (SIDS vs. SUD), the mechanism-based classification (SCD vs. SADS), and the overlap between SUDEP and SADS when arrhythmic mechanisms are involved. SUD: Sudden unexplained death; SCD: sudden cardiac death; SIDS: sudden infant death syndrome; SUDEP: sudden unexpected death in epilepsy; SADS: sudden arrhythmic death syndrome.
Given that SUD cases without specific pathological change are one of the major challenges in forensic practice, novel techniques for postmortem diagnosis or risk prediction are required to assist the identification of the COD. Molecular autopsy, which involves the analysis of genetic and molecular markers, represents a valuable approach for elucidating the underlying causes of these conditions[14]. Recently, modern high-throughput techniques, such as next-generation sequencing (NGS), mass spectrometry based multi-omics and magnetic resonance, assisted by artificial intelligence (AI) have been applied in biomarker discovery, etiological diagnosis and mortality risk alert. Increasing number of genetic variations has been discovered in diseases leading to SUD, especially in congenital arrhythmia including ion channelopathies[15-17]. In addition, in our previous studies, lipid biomarkers in cardiac tissues from SCD mouse model were identified by time-of-flight secondary ion mass spectrometry (ToF-SIMS), and extracellular vesicle based biomarkers including microRNAs (miRNAs), metabolites and proteins were validated for SCD diagnosis[18-20].
Modern forensic practical challenges require systematic integrity and logical coherence across all stages of evidence generation and interpretation in forensic practice. Therefore, further strengthening interdisciplinary research in forensic medicine has become urgent and essential. This review summarizes recent advances in the forensic investigation of SUD, with a focus on technical innovations including molecular autopsy, multi-omics approaches, virtual autopsy, and AI, aiming at elucidating the current advances of SUD with a particular focus on the technical innovations in forensic practice. With the advent of novel technical approaches, a growing proportion of SUDs are being resolved through definitive determination of the COD [Figure 2]. Despite the emergence of these advanced techniques, conventional autopsy including thorough macroscopic examination and systematic histopathological analysis remains the current gold standard for COD investigation[21,22], providing essential structural and morphological evidence that cannot be replaced by any single ancillary method[23].
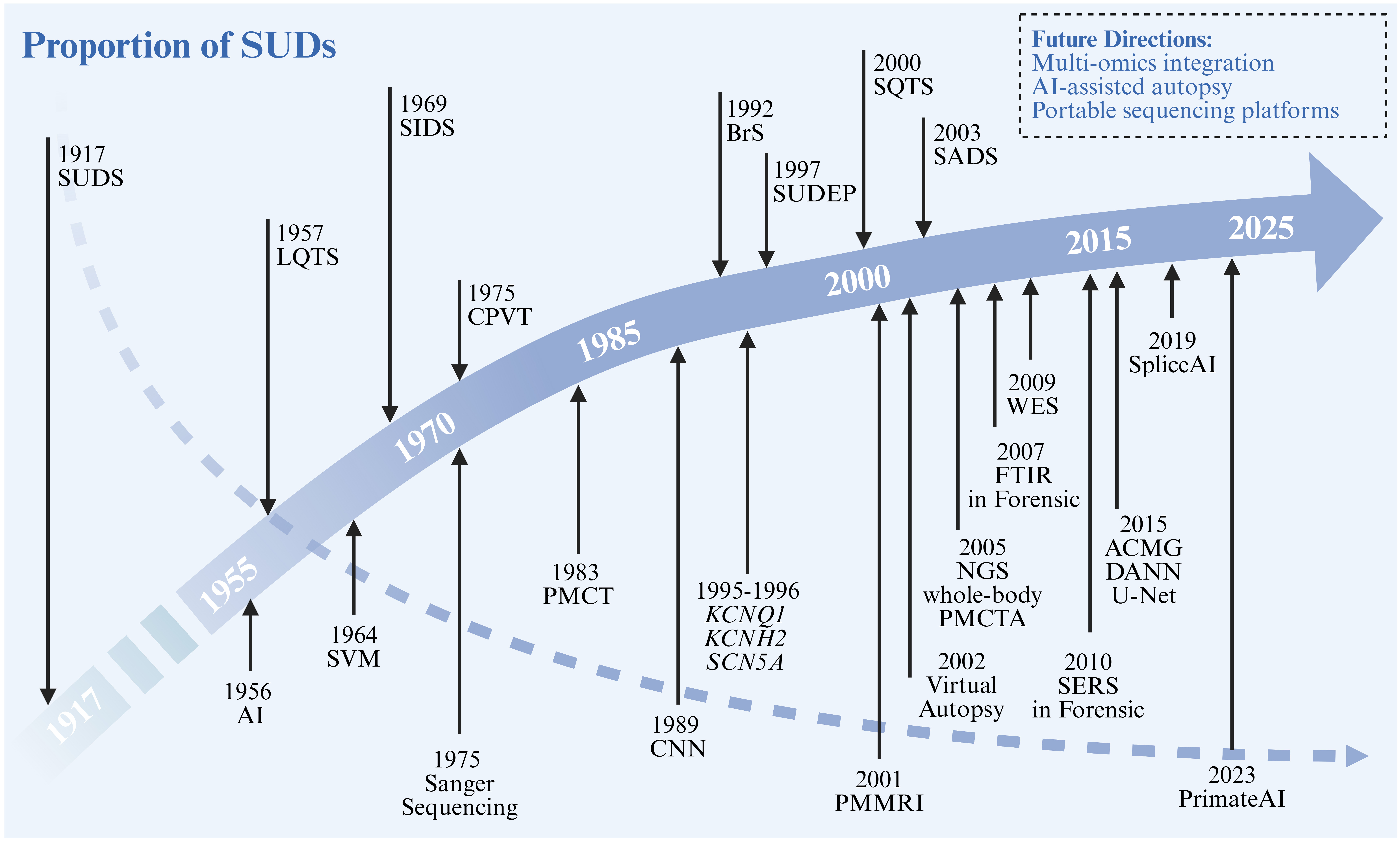
Figure 2. Conceptual timeline of major concepts and technique advances in SUDs. With the advancement of new technologies, the proportion of solved SUD cases has progressively increased over the past century. Solid arrow indicates the year that a concept or disease entity was first defined or formally named, or pathogenic gene was first reported in the literature. Gray dashed arrow indicates the downward trend in the proportion of SUDs. Created in BioRender. qi, M. (2026) https://BioRender.com/vxgvd6z. SUDS: Sudden unexplained death syndrome; LQTS: long QT syndrome; SIDS: sudden infant death syndrome; BrS: Brugada syndrome; CPVT: catecholaminergic polymorphic ventricular tachycardia; SUDEP: sudden unexpected death in epilepsy; SQTS: short QT syndrome; SADS: sudden arrhythmic death syndrome; AI: artificial intelligence; SVM: support vector machine; PMCT: postmortem computed tomography; CNN: convolutional neural network; PMMRI: postmortem magnetic resonance imaging; PMCTA: postmortem computed tomography angiography; NGS: next-generation sequencing; FTIR: Fourier transform infrared; WES: whole-exome sequencing; ACMG: American College of Medical Genetics and Genomics; DANN: deleterious annotation of genetic variants using neural networks.
MAJOR CAUSES RELATED TO SUDDEN UNEXPLAINED DEATHS
Cardiac channelopathy
Among all cardiovascular diseases, deleterious genetic alterations in cardiac ion channel proteins are characterized by the absence of distinct pathological alterations, yet they can give rise to life-threatening arrhythmias that often present as SCD. Hereditary primary electrical disorders, including long QT syndrome (LQTS), short QT syndrome (SQTS), Brugada syndrome (BrS), and catecholaminergic polymorphic ventricular tachycardia (CPVT), are known as cardiac channelopathies and account for up to 30% of all SCDs in the young[24], which are most commonly caused by mutations in genes encoding cardiac ion channels, receptors and/or their regulatory proteins[15,25]. While specific clinical and ECG features can identify patients at the highest risk of SCD, stratifying those at lower risk remains challenging, as their first clinical manifestation may be sudden cardiac arrest or SCD[26].
Genetic analyzing of deleterious genetic alterations of patients and their family members has become an important method for diagnosis of cardiac channelopathies in clinic[27], and may be an optional method in forensic identification. However, due to large amount of unknown genes and rare variants associated with channelopathies, and many previously reported variants seem to have disputed evidence in pathogenesis of channelopathies, genetic analysis is still not a routine method in the clinic and forensic practice in China yet. Based on the current Chinese expert consensus statement on SCD, genetic testing is recommended for SCD cases in clinic with a suspected inherited etiology to identify causative variants, facilitate cascade screening of at-risk relatives, and enable accurate etiological diagnosis[28]. In detail, for individuals with a defined cardiac phenotype, targeted gene panel testing focusing on well-established causative genes is preferred (Class I). In young (< 40 years) or phenotype-negative SCD cases with features suggestive of inherited arrhythmia syndromes (e.g., documented arrhythmic death or specific triggers), genetic evaluation focusing on primary arrhythmia syndrome genes, with optional inclusion of cardiomyopathy genes, is advised (Class I/IIa). Comprehensive postmortem sample collection (blood or fresh/fixed cardiac tissue) and multidisciplinary collaboration are emphasized to improve diagnostic yield, while the interpretation of variants of uncertain significance (VUS) requires caution and periodic re-evaluation[28]. Correspondingly, forensic guidelines also need to be updated to include genetic testing in cases of SUD.
Concealed cardiomyopathy
In the past 5 years, the concept of “concealed cardiomyopathy (CCM)” has emerged to address a critical subset of the cases lacking identifiable cardiac structural abnormalities after comprehensive macroscopic and microscopic examination, while deleterious alteration in a gene associated with cardiomyopathy was identified in postmortem genetic testing[29,30]. This entity highlights a crucial pathophysiological phase that malignant arrhythmias can occur prior to the development of overt structural changes in inherited cardiomyopathy[31].
In autopsy-inconclusive cohorts, the prevalence of CCM is considerable. In a landmark study, 15.4% (14/91) of autopsy-inconclusive SCD cases were attributed to CCM, with 70% of clinically actionable variants found in cardiomyopathy-associated genes and nearly two-thirds involving arrhythmogenic cardiomyopathy (ACM) genes[31]. The diagnostic yield was significantly higher in cases with subdiagnostic structural findings than in those with a completely normal heart. Postmortem genetic studies have detected pathogenic/likely pathogenic variants in up to 33% of young individuals diagnosed with myocarditis, suggesting inflammation can trigger lethal arrhythmias in genetically vulnerable myocardium[32]. Beyond the decedent, identifying a pathogenic or likely pathogenic variant enables cascade testing, as shown by 42.6% of first-degree relatives testing positive for the familial variant, of whom 65% exhibited an observable phenotype, while 27 genotype-negative relatives were released from follow-up[30,31].
In conclusion, CCM represents an under-recognized but clinically significant cause of SUDs, particularly in the young. Comprehensive evaluation should include not only a meticulous conventional autopsy but also broad, multi-phenotype genetic testing encompassing both ion channel and cardiomyopathy-associated genes, coupled with multidisciplinary family assessment[29,33].
Epilepsy
SUD in epilepsy (SUDEP) is a sudden and unexpected, and non-traumatic death of a person with epilepsy, occurring without a witnessed seizure, and without a toxicological or pathological cause detected during the postmortem examination[10,14]. SUDEP is a leading cause of mortality in epilepsy, accounting for up to 18% of deaths in patients with epilepsy[34]. Main mechanisms have been proposed for SUDEP: (1) cardiac dysfunction, including arrhythmias and other cardiac events; (2) respiratory factors, such as seizure-induced pulmonary dysfunction; (3) cerebral and autonomic nervous system dysregulation; and (4) some less frequent contributors including anti-epileptic drugs, vagal nerve stimulation, and genetic factors, such as rare variants in genes associated with increased susceptibility to SUDEP[35]. Seizure-induced apnea is a major event leading to death after generalized seizures[36]. Dravet syndrome, developmental and epileptic encephalopathy (DEE) and focal epilepsy are closely related to increasing risk of SUDEP[37].
The postmortem diagnosis of SUDEP is one of exclusion, relying primarily on witnessed seizures, medical records, and clinical history, and genetic testing has emerged as a highly effective tool in recent years. Over 33% of SUDEP cases are associated with deleterious genetic alterations in channelopathy-related genes, including some that are also implicated in SCD, such as variants in KCNH2 and SCN5A[38,39]. These variants may increase susceptibility to seizure-induced cardiorespiratory dysfunction or fatal arrhythmias[40]. Postmortem genetic findings allow for reclassification of the COD and enable cascade genetic screening of first-degree relatives, who may be at risk of inheritable cardiac channelopathies[41]. Moreover, knowledge of a genetic risk factor may guide anti-seizure medication choices (e.g., avoiding sodium channel blockers in patients with SCN1A or SCN8A variants)[42]. Therefore, genetic analysis should not be viewed solely as a research tool but rather integrated into SUDEP risk assessment and COD identification where available.
Sudden infant death syndrome
SIDS is now classified as SUD in the absence of both intrinsic and extrinsic risk factors[43]. The incidence of SIDS varies among studies, accounting for 42% to 66% of all infant deaths[44,45], and is typically higher between 2 and 4 months of age[46]. SIDS occurs in infants with no identifiable intrinsic health risks and no modifiable extrinsic factors related to the sleeping environment, that is, the infant’s position and location[47]. Given that deaths are often unobserved or unwitnessed, a standardized death-scene investigation is critical and recommended for establishing the COD to exclude any possibility of child abuse, unsafe products and environments[48]. Our current understanding of SIDS is predominantly derived from epidemiological studies conducted in Western countries, particularly Europe and North America. In China, there is a paucity of reported SIDS cases, and neither clinical guidelines nor expert consensus statements on SIDS are currently available.
Increasing evidence has shown that SIDS shares common molecular and pathophysiological mechanisms with SADS and SUDEP, particularly involving cardiac arrhythmias[14]. Other genetic background, such as rare variants in genes associated with inherited metabolic conditions, immune dysfunction and nicotine response, may also play a causal role in SIDS[49], necessitating molecular autopsy including genetic analysis for elucidation of COD.
Postmortem decomposition
Postmortem decomposition, particularly putrefaction, poses substantial challenges in forensic pathology by progressively degrading tissues and obscuring critical morphological and biochemical evidence. The ability to determine an accurate COD is severely compromised in decomposed bodies, primarily due to the loss of histoarchitectural integrity, the introduction of postmortem artifacts, and the limitations imposed on conventional and advanced diagnostic techniques. In previous studies, putrefactive changes significantly impair the forensic evaluation of cardiac pathology. Critical diagnostic features are often lost: conventional histology of the myocardium is frequently unreliable due to autolysis and bacterial overgrowth, and myocardial wall thinning caused by putrefaction may mimic dilated cardiomyopathy, creating a substantial risk of misinterpretation[50]. Radiological techniques are also hindered by decomposition artifacts, including gas accumulation, vascular collapse, and fluid shifts, all of which impair visualization of coronary arteries. Currently, no standardized forensic methodology exists to consistently differentiate antemortem cardiac pathology from postmortem artifacts[51].
To define Post-Mortem Diagnostic Uncertainty, Van Den Bogaert et al. classify putrefaction as “lack of data due to post-mortem changes and destructive forces”, under which conditions conventional histological and toxicological analyses often fail. In cases of advanced decomposition, certain investigations become impractical or impossible, and unlike incomplete autopsies, such data loss is beyond the control of the forensic pathologist[52]. Moreover, conditions without morphological abnormalities (e.g., channelopathies) remain a persistent source of uncertainty, as decomposition destroys even the limited structural evidence that might otherwise be present[50].
In summary, putrefaction profoundly complicates COD determination by degrading diagnostic substrates and introducing artifacts. However, by recognizing both the persistent features (such as calcified plaques) and the limitations of standard techniques, forensic pathologists can still derive valuable information. Structured uncertainty communication and the adoption of validated ancillary methods are essential steps toward improving diagnostic accuracy in decomposed bodies[52].
MOLECULAR AUTOPSY IN SUDDEN UNEXPLAINED DEATH
One of the most significant advances in the investigation of SUD has been the emergence of molecular autopsy, defined as the application of postmortem genetic testing to identify pathogenic variants[53]. It is important to emphasize, however, that molecular autopsy serves as a complementary approach rather than a replacement for conventional autopsy. While conventional autopsy and histopathological examination remain essential components of forensic investigation, they are inherently limited in their ability to detect electrical disturbances or molecular abnormalities, which frequently underlie SUDs.
Over the past decade, rapid developments in NGS technologies have substantially broadened the scope of postmortem genetic analysis[53,54]. Until today, the number of genes with a definite association with cardiac channelopathies remains limited. Targeted gene panel sequencing often suffices for clinical diagnostic purposes and yields the highest diagnostic rate with the fewest VUS. However, cases with negative results of genetic testing remain a problem in both clinical and forensic practice. To address these cases, approaches have evolved from targeted gene panels to more comprehensive strategies, including whole-exome sequencing (WES) and whole-genome sequencing (WGS), enabling systematic interrogation of genetic contributors such as cardiac channelopathies and cardiomyopathies in cases of SUD. Data show that the diagnostic yield increases from approximately 20% with Sanger sequencing to 35% or higher with targeted NGS[55]. However, analyzing more genes does not automatically translate into higher diagnostic yield; rather, broader approaches such as WES and WGS may increase the detection of incidental findings and VUS, complicating interpretation and genetic counseling[56]. These comprehensive strategies should therefore be prioritized for research settings or for cases with high clinical suspicion but negative panel testing, where novel gene discovery or detection of non-coding variants is warranted.
Importantly, the value of molecular autopsy extends beyond establishing the COD. The identification of clinically actionable variants facilitates cascade screening among surviving relatives, allowing for genetic counseling, clinical monitoring, and implementation of preventive strategies[57]. Family-based investigations following autopsy-negative sudden death may help uncover previously unrecognized carriers, thereby reducing the risk of further fatal events.
Sanger sequencing
Early applications of molecular autopsy predominantly relied on Sanger sequencing to analyze a limited number of pathogenic variants in key arrhythmia-related genes[55], which remains the gold standard for DNA sequencing due to its high accuracy and reliability. According to current guidelines[58], several genes associated with SCD can be effectively analyzed using Sanger sequencing, such as KCNQ1, KCNH2, SCN5A, RYR2, and LMNA[10,58]. These genes are commonly implicated in inherited arrhythmia syndromes and cardiomyopathies and were the primary targets in early molecular autopsy studies. Moreover, Sanger sequencing also serves as the gold standard for targeted cascade genetic testing of at-risk first-degree relatives, enabling rapid and cost-effective determination of carrier status to guide clinical surveillance and preventive interventions[59]. With the rapid expansion in the number of genes linked to SUD, Sanger sequencing is increasingly limited by its low throughput and inefficiency in analyzing large gene sets. Consequently, NGS technologies have progressively replaced Sanger sequencing as the primary discovery tool, owing to their high-throughput capacity and scalability[53]. In current practice, Sanger sequencing is more commonly used as a confirmatory method for validating variants identified through NGS.
Next-generation sequencing
The emergence of NGS technologies has fundamentally transformed the analytical capacity of molecular autopsy, enabling high-throughput and cost-effective interrogation of genetic variation on an unprecedented scale[53,54]. By allowing massively parallel sequencing of millions of DNA fragments, NGS has shifted postmortem genetic analysis from limited, hypothesis-driven testing toward more comprehensive and systematic approaches[60]. NGS-based strategies can be implemented at multiple levels, including targeted gene panels, WES, and WGS, each offering distinct advantages depending on the clinical or forensic context.
Targeted gene panels
Targeted gene panels represent the most widely adopted approach, focusing on curated sets of genes with well-established associations to inherited arrhythmia syndromes and cardiomyopathies. Panel-based testing achieves high coverage, cost efficiency, and relatively straightforward interpretation. This makes it particularly suitable in cases of SCD where a cardiac etiology is strongly suspected, as a limited number of well-characterized genes account for a substantial proportion of inherited arrhythmia syndromes and cardiomyopathies. Multiple studies have demonstrated that disease-oriented gene panels targeting key SUD-related genes - such as KCNQ1, KCNH2, SCN5A, RYR2, MYH7, and TTN - can effectively identify pathogenic or likely pathogenic variants in a significant subset of cases[61,62].
Whole-exome sequencing
WES selectively captures and sequences the protein-coding regions of the genome, which account for approximately 1% ~ 2% of the total genomic content but harbor the majority of known disease-causing variants[54]. In the context of postmortem investigation, WES is particularly advantageous as it can be applied to fragmented DNA samples and enables simultaneous analysis of a large number of genes without requiring prior selection of specific targets. Therefore, WES has become a widely adopted approach in molecular autopsy, especially in cases where targeted gene panel testing is inconclusive or when the underlying phenotype is unclear[53,62]. It allows for the exploration of both known and novel genes associated with SUD, including conditions beyond classical cardiac channelopathies[62], thereby expanding the diagnostic spectrum. In addition, WES avoids the need for repeated sequencing as new candidate genes emerge, making it a flexible and efficient strategy for large-scale genetic investigation. The expanded scope of WES also results in the identification of a substantial number of genetic variants, many of which lack sufficient evidence for definitive classification and are therefore categorized as VUS[63]. This introduces considerable challenges in interpretation and may lead to diagnostic ambiguity.
Whole-genome sequencing
Unlike WES which is restricted to exonic sequences, WGS does not require prior target enrichment and instead captures all genomic DNA fragments, followed by massively parallel sequencing and alignment to a reference genome. This approach allows for the detection of a wide spectrum of genetic variation, including single nucleotide variants, insertions and deletions, structural variants, and alterations within regulatory elements such as promoters, enhancers, and untranslated regions[54,64]. In postmortem settings, WGS provides a more complete representation of the genetic landscape, which is particularly relevant for uncovering mechanisms that may not involve protein-coding regions[53,60]. The routine application of WGS is currently limited by higher costs, increased computational requirements, and the substantial complexity of data interpretation. Moreover, the vast number of variants identified - including those located in poorly annotated non-coding regions - further amplifies the challenge of distinguishing clinically relevant findings, reinforcing the importance of integrative analytical frameworks.
Variant interpretation in molecular autopsy
Given the large number of variants identified in each individual, systematic filtering represents a critical first step. Technical filtering is applied to minimize false-positive calls arising from sequencing or alignment errors, commonly using thresholds such as a minimum read depth (e.g., ≥ 30×) and variant allele frequency (e.g., ≥ 20%). Subsequently, biological filtering is performed to distinguish rare, potentially relevant variants from background genetic noise. This process typically incorporates population frequency data, where variants with a minor allele frequency below 0.1% are prioritized, alongside consideration of gene relevance, particularly those previously associated with inherited arrhythmia syndromes or cardiomyopathies[64].
Following filtering, variant prioritization aims to assess the potential functional and clinical significance of the remaining candidates[65,66]. Public databases such as ClinVar and OMIM and in silico prediction tools including SIFT, PolyPhen-2, and MutationTaster are widely used to estimate the potential impact of variants on protein structure and function. Evolutionary conservation analysis further refines prioritization, as variants affecting highly conserved residues or domains are more likely to be functionally significant. To standardize variant interpretation, the American College of Medical Genetics and Genomics (ACMG), in collaboration with the Association for Molecular Pathology (AMP), has established a widely adopted five-tier classification system, categorizing variants as pathogenic, likely pathogenic, VUS, likely benign, or benign[65]. This framework integrates multiple lines of evidence, including population data, computational predictions, functional assays, and segregation information, enabling a structured and transparent evaluation process. According to the ACMG/AMP guidelines, pathogenic and likely pathogenic variants are defined as deleterious, disease-causing alterations supported by sufficient evidence across multiple domains including population frequency, computational prediction, functional assays, and segregation data, whereas VUS indicates insufficient or conflicting evidence to determine their clinical effect and are considered non-actionable for clinical management or cascade testing[67].
In the investigation of SUD, a stepwise genetic testing strategy is generally recommended[61,62,68,69]. Targeted gene panels focusing on genes closely related to the suspected phenotype are often used as a first-line approach. While pathogenic/likely pathogenic variants provide actionable results that warrant cascade genetic screening in relatives, VUS findings represent a major interpretative dilemma because post-mortem tissues preclude functional validation, segregation analysis, and phenotypic correlation in the deceased proband[70]. Given the large number of variants identified through NGS, variant interpretation has become a critical step, requiring careful filtering, prioritization, and classification within established frameworks. Importantly, the integration of molecular findings with clinical and familial information substantially enhances interpretative accuracy[54,71]. For molecular autopsy specifically, international recommendations advocate that all rare variants identified in inherited arrhythmic syndrome genes be urgently reclassified following ACMG guidelines, with empirical studies showing that over 90% of previously unstandardized rare variants modified their classification upon rigorous ACMG application, and a maximum reanalysis interval of five years has been proposed to incorporate evolving evidence from population databases, case reports, and in silico tools[53]. Ultimately, accurate interpretation of rare variants after molecular autopsy necessitates an experienced multidisciplinary team and adherence to standardized forensic guidelines, given that misinterpretation of VUS may lead to inaccurate genetic diagnoses and inappropriate therapeutic interventions in surviving relatives[70].
We summarized representative SUD-related genes primarily on the basis of ClinGen gene-disease validity classifications, prioritizing genes with definitive, strong, or moderate evidence for disease causation in Figure 3. Representative pathogenic variants in arrhythmia-associated genes and their evidence scores are shown in Table 1. Representative examples of genetic variants in KCNQ1 classified according to the ACMG/AMP five-tier system are shown in Table 2.
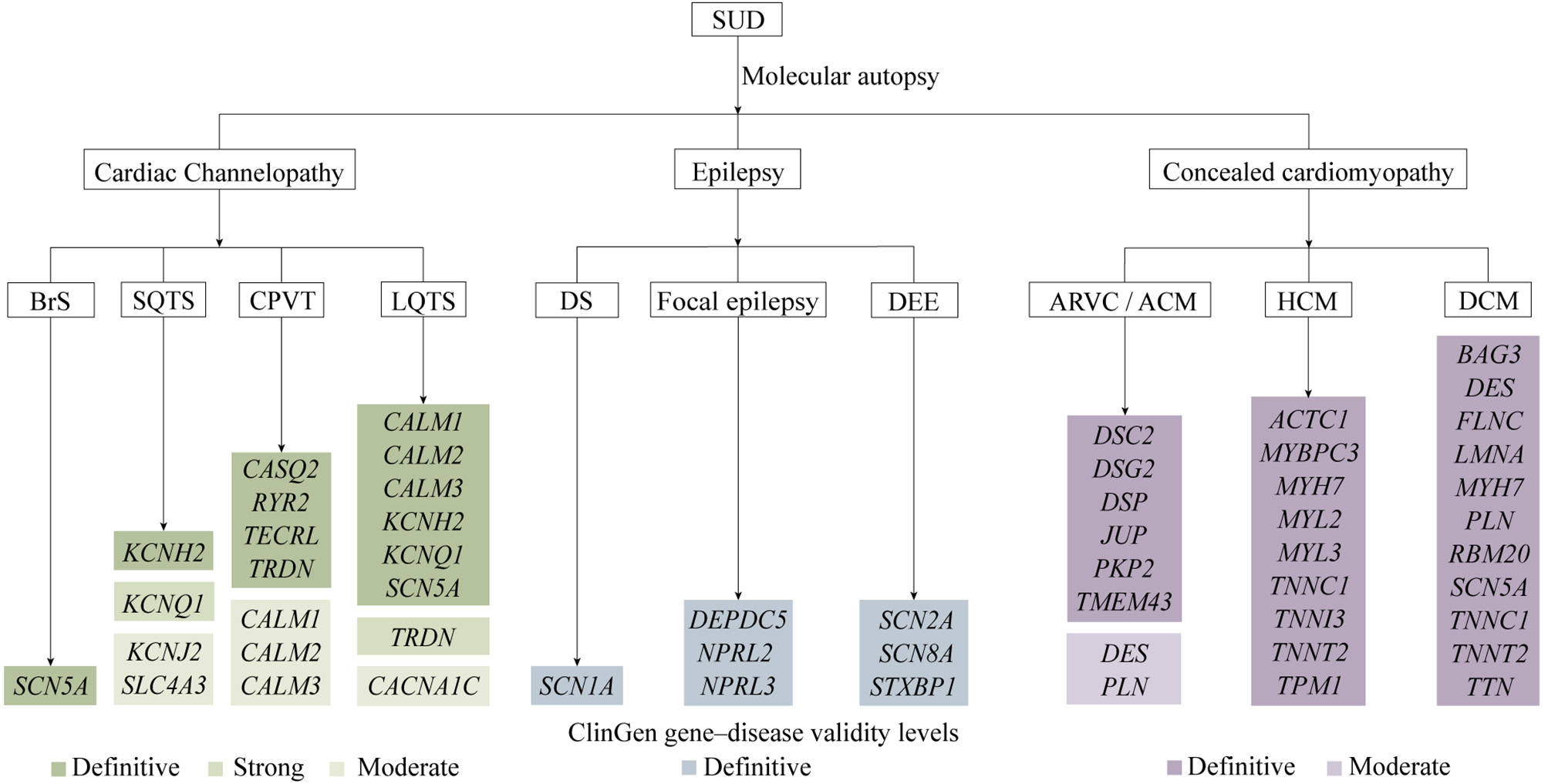
Figure 3. Summary of genes associated with conditions contributing to SUD[72-80]. SUD: Sudden unexplained death; BrS: Brugada syndrome; SQTS: short QT syndrome; CPVT: catecholaminergic polymorphic ventricular tachycardia; LQTS: long QT syndrome; DS: Dravet syndrome; DEE: developmental and epileptic encephalopathy; ARVC: arrhythmogenic right ventricular cardiomyopathy; ACM: arrhythmogenic cardiomyopathy; HCM: hypertrophic cardiomyopathy; DCM: dilated cardiomyopathy.
Summary of representative pathogenic variants in arrhythmia-associated genes and their evidence scores
| Transcript | Gene | cDNA change | Protein change | Disease | Inheritance pattern | Total score | Evidence codes and scores | Supporting references |
| NM_000218.3 | KCNQ1 | c.1032G>A | p.Ala344= | LQTS | AD | 11 | PS3(4)+PS4(4)+PM2(1)+PP3(1)+PP4(1) | [81,82] |
| NM_000218.3 | KCNQ1 | c.1766G>A | p.Gly589Asp | LQTS/JLNS | AD/AR | 11 | PS3(4)+PS4(4)+PM2(1)+PP3(1)+PM3(1) | [83,84] |
| NM_000238.4 | KCNH2 | c.1810G>A | p.Gly604Ser | LQTS | AD | 12 | PS3(4)+PS4(2)+PM2(1)+PP1(4)+PP3(1) | [85,86] |
| NM_000238.4 | KCNH2 | c.1882G>A | p.Gly628Ser | LQTS | AD | 11 | PM6(1)+PS3(4)+PS4(4)+PM2(1)+PP3(1) | [87,88] |
| NM_000238.4 | KCNH2 | c.2775dup | p.Pro926AlafsTer14 | LQTS | AD | 14 | PVS1(8)+PS4(2)+PP1(4) | [89] |
| NM_000238.4 | KCNH2 | c.1853C>T | p.Thr618Ile | SQTS | AD | 14 | PS3(4)+PS4(4)+PM2(1)+PP1(4)+PP3(1) | [90,91] |
| NM_000719.7 | CACNA1C | c.1216G>A | p.Gly406Arg | LQTS | AD | 13 | PM6(4)+PS3(4)+PS4(4)+PP3(1) | [92,93] |
| NM_000335.5 | SCN5A | c.3282G>A | p.Trp1094Ter | BrS | AD | 11 | PVS1(8)+PS4(2)+PM2(1) | [94,95] |
| NM_000335.5 | SCN5A | c.1603C>T | p.Arg535Ter | BrS | AD | 11 | PVS1(8)+PS4(2)+PP1(1) | [96,97] |
| NM_000335.5 | SCN5A | c.5347G>A | p.Glu1783Lys | LQTS/BrS | AD | 13 | PS3(4)+PS4(4)+PP1(4)+PP3(1) | [98,99] |
| NM_001232.4 | CASQ2 | c.62del | p.Glu21GlyfsTer15 | CPVT | AR | 10 | PVS1(8)+PM2(1)+PM3(1) | [100,101] |
| NM_001232.4 | CASQ2 | c.919G>C | p.Asp307His | CPVT | AR | 13 | PS3(4)+PS4(2)+PM2(1)+PM3(1)+PP1(4)+PP3(1) | [102,103] |
| NM_001010874.5 | TECRL | c.658-2A>G | p.? (splice acceptor) | CPVT | AR | 10 | PVS1(8)+PM2(1)+PM3(1) | [104] |
| NM_001035.3 | RYR2 | c.1259G>A | p.Arg420Gln | CPVT | AD | 12 | PS3(4)+PS4(2)+PM2(1)+PP1(4)+PP3(1) | [105,106] |
| NM_006073.4 | TRDN | c.22+1G>T | p.? (splice donor) | LQTS/CPVT | AR | 10 | PVS1(8)+PM2(1)+PM3(1) | [107] |
Representative KCNQ1 variants across ACMG/AMP classifications and their evidence scores
| Transcript | Gene | cDNA change | Protein change | Disease | Inheritance pattern | ACMG/AMP classification | Total score | Evidence codes and scores | Supporting references |
| NM_000218.3 | KCNQ1 | c.1927G>A | p.Gly643Ser | LQTS | AD | Benign | N/A | BA1 | |
| NM_000218.3 | KCNQ1 | c.1343C>G | p.Pro448Arg | LQTS | AD | Benign | N/A | BA1 | |
| NM_000218.3 | KCNQ1 | c.514G>A | p.Val172Met | LQTS | AD | Benign | -10 | BS1(-4)+BS4(-4)+BS3(-2) | [108,109] |
| NM_000218.3 | KCNQ1 | c.840G>T | p.Val280= | LQTS | AD | Likely Benign | -2 | BP4(-1)+BP7(-1) | |
| NM_000218.3 | KCNQ1 | c.1252G>A | p.Val418Ile | LQTS | AD | Likely Benign | -4 | BS1(-4) | |
| NM_000218.3 | KCNQ1 | c.458C>T | p.Thr153Met | LQTS | AD | Likely Benign | -5 | BS1(-4)+BP5(-1) | [110] |
| NM_000218.3 | KCNQ1 | c.590C>T | p.Pro197Leu | LQTS | AD | Uncertain Significance | 1 | PP3(1) | |
| NM_000218.3 | KCNQ1 | c.776G>A | p.Arg259His | LQTS | AD | Uncertain Significance | 2 | PS3(1)+PP3(1) | [111,112] |
| NM_000218.3 | KCNQ1 | c.1120C>T | p.Leu374Phe | LQTS | AD | Uncertain Significance | 2 | PM2(1)+PP3(1) | |
| NM_000218.3 | KCNQ1 | c.565G>A | p.Gly189Arg | LQTS | AD | Uncertain Significance | 5 | PS3(2)+PS4(1)+PM2(1)+PP3(1) | [113,114] |
| NM_000218.3 | KCNQ1 | c.958C>T | p.Pro320Ser | LQTS | AD | Uncertain Significance | 5 | PS4(1)+PM1(2)+PM2(1)+PP3(1) | [115,116] |
| NM_000218.3 | KCNQ1 | c.1096C>T | p.Arg366Trp | LQTS | AD | Likely Pathogenic | 6 | PS4(4)+PM2(1)+PP3(1) | [117,118] |
| NM_000218.3 | KCNQ1 | c.477+5G>A | p.? (splice region) | LQTS | AD | Likely Pathogenic | 6 | PS4(4)+PP3(1)+PP4(1) | [119,120] |
| NM_000218.3 | KCNQ1 | c.1552C>T | p.Arg518Ter | LQTS | AD | Likely Pathogenic | 8 | PVS1(8) | |
| NM_000218.3 | KCNQ1 | c.176del | p.Pro59GlnfsTer27 | LQTS | AD | Likely Pathogenic | 9 | PVS1(8)+PM2(1) | |
| NM_000218.3 | KCNQ1 | c.674C>T | p.Ser225Leu | LQTS | AD | Likely Pathogenic | 9 | PS3(4)+PS4(4)+PP3(1) | [121,122] |
MULTI-OMICS APPROACHES IN SUD
Proteomics
Proteomics is the systematic study of protein expression, structure, and function within biological systems, and can reflect the underlying pathophysiological state prior to death and therefore hold significant forensic relevance[123]. Over the past decades, proteomic technologies have evolved from early separation-based approaches to high-throughput analytical platforms centered on mass spectrometry.
Liquid chromatography-tandem mass spectrometry
Liquid chromatography-tandem mass spectrometry (LC-MS) is currently the core technology in proteomics research, offering high sensitivity and throughput, and allowing the simultaneous detection of a large number of proteins in complex biological samples, and has become the primary platform for proteomic studies in SUD[123].
Sequential window acquisition of all theoretical fragment ion spectra
Sequential window acquisition of all theoretical fragment ion spectra (SWATH) is a high-resolution mass spectrometry technique based on a data-independent acquisition strategy[123-125]. Compared with conventional mass spectrometry approaches, SWATH is particularly suitable for quantitative proteomics of complex biological samples, as well as for the detection of low-abundance proteins and post-translational modifications. SWATH has been used to identify and quantify proteins differentially expressed between healthy individuals and patients and showed advantages in forensic toxicology[126,127].
Protein Biomarkers
Protein biomarkers remain the cornerstone of biochemical investigation in SCD. Commonly used markers include cTnI and cTnT, creatine kinase-MB (CK-MB), heart-type fatty acid-binding protein (H-FABP), glycogen phosphorylase isoenzyme BB (GPBB), lactate dehydrogenase (LDH), myoglobin, ischemia-modified albumin (IMA), and inflammatory markers such as C-reactive protein (CRP)[123]. Among these, cardiac troponins are widely regarded as the gold standard for detecting myocardial necrosis due to their high cardiac specificity and sensitivity, with demonstrated diagnostic value in both pericardial fluid and peripheral blood[128-130]. CK-MB, although limited by lower specificity due to skeletal muscle interference, may provide additional diagnostic value when interpreted in combination with troponins[131,132]. Early ischemic markers such as H-FABP and GPBB are particularly useful in cases with very short survival times, as they are rapidly released following myocardial injury[133]. The interpretation of these biomarkers in postmortem settings is complicated by factors such as postmortem interval, hemolysis, and sample heterogeneity. Consequently, a multi-marker approach is generally considered more reliable than single-analyte analysis. In recent years, novel biomarkers of myocardial ischemia have been reported, but their application in postmortem forensic investigations remains unsupported by empirical data.
Galectin-3 (Gal-3) is a β-galactoside-binding lectin secreted primarily by activated macrophages and is associated with inflammation and myocardial fibrosis. Elevated Gal-3 levels have been linked to adverse remodeling and poor prognosis in chronic HF. Gal-3 may serve as an indicator of underlying fibrotic cardiac remodeling, offering insight into structural substrates that predispose to fatal arrhythmias[134,135].
Copeptin is released in equimolar amounts with arginine vasopressin (AVP) during physiological stress. Copeptin has been proposed as a marker of acute endogenous stress response and, when combined with cardiac troponins, may improve the early detection of acute myocardial events, although its standalone diagnostic value remains limited[136].
Cardiac myosin-binding protein C (cMyBP-C) is a structural protein of the sarcomere that plays a key role in regulating myocardial contraction. It is rapidly released into circulation following myocardial injury and has demonstrated high cardiac specificity. Recent studies suggest that cMyBP-C may be a sensitive biomarker for early myocardial damage[60,66], potentially outperforming traditional markers in certain contexts, making it a promising candidate for forensic diagnosis of acute cardiac death.
Selenium-binding protein 1 (SELENBP1) and vinculin (VCL) have recently been investigated in cases of sudden death associated with coronary artery spasm[137].
SELENBP1 is involved in cellular redox regulation, while VCL plays a role in cytoskeletal integrity and cell adhesion. Studies have demonstrated that SELENBP1 exhibits high sensitivity and specificity, whereas VCL provides additional discriminatory value, suggesting their potential utility as novel biomarkers in specific subtypes of SCD[137].
Pentraxin-3 (PTX3) is an acute-phase protein produced by macrophages and vascular endothelial cells in response to inflammation, reflecting local vascular inflammation and associated with atherosclerotic plaque instability and thrombosis. Elevated PTX3 levels indicate acute coronary events[137,138], particularly in cases where histological evidence is limited, providing additional support for the diagnosis of ischemic death.
Metabolomics
Metabolomics focuses on the comprehensive analysis of small-molecule metabolites within biological systems, typically reflecting the downstream outcomes of gene expression and protein activity. Current metabolomics studies in death and diseases are primarily based on analytical platforms such as LC-MS, gas chromatography-mass spectrometry (GC-MS), and nuclear magnetic resonance (NMR), which enable the detection and quantification of a broad range of endogenous metabolites[139-141]. These techniques allow for the characterization of metabolic alterations associated with cardiac dysfunction, hypoxia, electrolyte imbalance, and other pathophysiological processes that may contribute to sudden death.
Hypoxia/ischemia (e.g., cerebral ischemia, myocardial infarction) induces metabolic dysfunction, alters amino acid profiles (e.g., decreased glycine, isoleucine, lysine), shifts metabolism to anaerobic glycolysis, causing lactate and pyruvate accumulation in postmortem fluids, and triggers oxidative stress and ROS[142,143]. These metabolites serve as key evidence supporting diagnosis of ischemic causes of death and asphyxia[123,144-147]. Though non-specific, these changes support forensic diagnosis of systemic stress and ischemia when interpreted alongside other metabolic markers[148,149].
Metabolomics provides functional molecular evidence for SUD cases with negative conventional autopsies by capturing terminal metabolic fingerprints of hypoxia, oxidative stress, and systemic inflammation. Although individual metabolite changes lack specificity, integrating multi-marker panels through machine learning (ML) algorithms and combination with molecular autopsy can effectively support the differential diagnosis of ischemic causes of death, asphyxia, and endogenous stress-triggered events[150]. Specific metabolite panels have shown promise in distinguishing SCD from other causes of death. For instance, alterations in the kynurenine pathway (e.g., increased kynurenine/tryptophan ratio) have been observed in SCD cases, reflecting inflammation and oxidative stress[151,152]. A recent study identified a combination of pyruvate, L-threonic acid, and N-acetyl-L-cysteine as a potential signature for ACS-related sudden death, with improved discriminatory power compared to any single metabolite[153]. ML has been increasingly integrated with metabolomics to enhance forensic classification. For example, supervised ML algorithms such as random forest and support vector machines (SVM) have been trained on postmortem metabolomics profiles to discriminate between SCD, asphyxia, and poisoning, achieving high accuracy[154,155]. A large-scale study of 4,282 human postmortem cases demonstrated that orthogonal partial least squares discriminant analysis (OPLS-DA) models could discriminate five COD groups (acidosis, drug intoxication, hanging, ischemic heart disease, and pneumonia) with specificity-optimized prediction accuracies ranging from 73% to 99%[156]. These approaches can identify complex, non-linear metabolic signatures that are not detectable by univariate analysis. In SUD cases, ML-assisted metabolomics may help uncover distinct metabolic fingerprints associated with channelopathies, concealed cardiomyopathies, or epileptic seizures, offering a novel avenue for postmortem diagnosis. Metabolomics facilitates a multi-omics integration framework that transforms SUD from a diagnosis of exclusion into a precision-based assessment supported by objective pathophysiological evidence, addressing critical gaps in conventional forensic evaluation of SUDs.
Transcriptomics
Transcriptomics allows the investigation of functional changes at the gene expression level. Dysregulation of genes encoding ion channel proteins may contribute to electrical instability and increase susceptibility to fatal arrhythmias[157]. In addition, transcriptional changes associated with fibrosis, inflammation, and apoptosis suggest that subtle molecular remodeling may precede overt structural abnormalities detectable by conventional autopsy[158].
Non-coding RNAs - particularly miRNAs - have emerged as highly promising candidates for forensic applications. Due to the tissue specificity and relative stability in postmortem tissues and body fluids, miRNAs serve as ideal biomarkers in forensic investigations. Several cardiac-enriched miRNAs, such as miR-1, miR-133, miR-208, and miR-499, have been shown to be significantly upregulated in cases of ischemic sudden death and correlate with established markers of myocardial injury and histological evidence of necrosis[159,160]. Importantly, distinct miRNA expression profiles may enable differentiation between ischemic SUD and primary arrhythmic deaths without structural abnormalities, providing valuable support in autopsy-negative cases[160]. High-throughput sequencing and quantitative PCR studies have demonstrated that miRNA profiles remain stable for up to 196 h postmortem, reinforcing their reliability as postmortem biomarkers[161]. Moreover, the analysis of extracellular vesicles has shown enhanced diagnostic performance compared to circulating miRNAs alone[18,162]. Encapsulation within vesicles protects nucleic acids from degradation and may preserve disease-specific molecular signatures, enabling improved discrimination between ischemic and non-cardiac COD, as well as between different cardiac pathologies.
Current available biomarkers of SCD, SIDS are listed in Table 3. Although no specific biomarker for SUDEP has been reported so far, several promising candidates are under active investigation. Potential biomarkers include circulating neuropeptides (e.g., substance P, neuropeptide Y) reflecting autonomic dysregulation, inflammatory markers (e.g., IL-6, TNF-α) associated with seizure-induced neuroinflammation, and miRNA signatures (e.g., miR-134, miR-146a) linked to neuronal excitability and seizure severity[173-175]. Future multi-omics studies are expected to identify and validate SUDEP-specific biomarkers that could aid in risk stratification and forensic diagnosis.
Selected diagnostic biomarkers of SUD.
| Classification | Selected Biomarkers | References |
| SCD | Protein: Cardiac troponin I/T (cTnI/T) , Myoglobin (Myo), Creatine kinase-MB (CK-MB), C5b-9 (MAC), Heart fatty acid-binding protein (H-FABP), GAL-3, NT-proBNP, IMA, GPBB, LDHB, cMyBP-C, SELENBP1, VCL, and PTX3 Nucleic acids: Heart-specific miRNAs (hsa-miR-1, -133, -208, -499), circSLC8A1, and circNFIX Metabolites: Pyruvate, L-threonic acid, and N-acetyl-L-cysteine | [10,18,20,66,128-135,137,138,157-160,162-164] |
| SIDS | Protein: Fetal hemoglobin, IL-6, tryptase, and serotonin receptors Enzyme: Butyrylcholinesterase (BChE) activity Metabolite: Serotonin, hypoxanthine, ornithine, 5-hydroxylysine, 1-stearoyl-2-linoleoyl-GPC (18:0/18:2), ribitol, and arabitol/xylitol | [165-172] |
| SUDEP | No relevantly diagnostic biomarkers were reported | N/A |
Raman spectroscopy
Raman spectroscopy is a label-free vibrational spectroscopic method that reflects the biochemical composition of biological samples through inelastic light scattering[176]. Surface-enhanced Raman spectroscopy (SERS) is more suitable for detecting low-abundance targets in complex biological samples for its sensitivity[177]. In SUD, Raman-based analysis may help identify subtle biochemical changes[123,178,179], and may be used for rapid molecular profiling of tissues and body fluids and therefore complement conventional biomarkers[123,176]. Unlike conventional assays that focus on individual analytes, Raman spectra reflect broader molecular changes and may provide a more integrated view of the perimortem biochemical state[180]. This is consistent with recent studies of SERS-based cardiac biomarker profiling, in which multiplex platforms have enabled simultaneous assessment of several serum cardiac markers and improved molecular characterization of cardiovascular risk states[177,181,182].
Our recent studies have shown that SERS-based platforms can be used for cross-category biomarker detection and early warning of SCD[183]. These findings indicate that Raman-derived molecular fingerprints may be useful in the combined assessment of different biomarker classes in sudden cardiac events[183,184]. At present, however, the forensic application of Raman spectroscopy in SUD remains limited. Major constraints include matrix interference, postmortem degradation, signal reproducibility, and the lack of standardized forensic reference databases[123,178]. Raman spectroscopy is therefore better regarded as a supplementary technique than as an independent diagnostic method in the forensic investigation of SUD[185,186].
Fourier transform infrared spectroscopy techniques
Fourier transform infrared (FTIR) spectroscopy techniques have emerged as a powerful, label-free tool for forensic death investigation by capturing subtle biochemical alterations that are often undetectable by conventional autopsy. It has been successfully applied to identify key biomarkers in a restraint stress model, and differentiate COD such as asphyxia from sudden cardiac arrest[187]. When combined with ML algorithms, FTIR enables objective and high-throughput classification of postmortem samples, offering a complementary approach to traditional histology[188-190]. Furthermore, the application of attenuated total reflection (ATR)-FTIR to biofluids (serum, plasma, urine) provides a non-invasive “fluid biopsy” strategy to assess systemic metabolic disturbances[188,191], making it particularly valuable for cases where tissue samples are limited or ambiguous, such as in SUD. These integrated spectroscopic and computational strategies hold promise for transforming forensic pathology by providing rapid, objective, and molecularly grounded evidence for COD determination.
VIRTUAL AUTOPSY
PMCT
Postmortem computed tomography (PMCT) has become one of the most widely used imaging modalities in forensic practice[192]. Because SUD is the absence of a definitive COD after conventional autopsy and histological examination, the primary value of PMCT lies in refining the diagnostic process through exclusion, guidance, and supportive findings. The key contributions of PMCT in SUD investigations are the systematic exclusion of alternative COD that may be subtle, atypical, or easily overlooked during conventional autopsy. Postmortem gas formation, livor mortis, tissue density changes, vascular integrity loss, and fluid redistribution can all alter CT imaging characteristics over time, potentially leading to misinterpretation[192,193]. In SUD cases, especially those involving suspected infection or metabolic disturbances such as diabetic ketoacidosis, specific gas distribution patterns may provide important clues[193,194]. PMCT also plays an important role in excluding external causes that may mimic SUD. For example, in drowning cases, PMCT may demonstrate characteristic findings such as fluid accumulation in the airways and paranasal sinuses, ground-glass opacities in the lungs, pulmonary hyperinflation, and retention of foam-like material within the airways[195]. In cases where arrhythmogenic cardiomyopathies or other subtle myocardial abnormalities are suspected, PMCT may reveal indirect or localized changes in myocardial structure, such as areas of altered density that could correspond to fibrofatty replacement[196,197]. Although these findings are often insufficient for definitive diagnosis, they can provide valuable guidance for focused histological sampling and molecular investigations, including genetic testing. This targeted approach is particularly important in SUD, where diffuse or non-specific sampling may fail to detect localized pathological substrates. In this way, PMCT contributes to a more structured and hypothesis-driven investigation process.
Despite these advantages, PMCT has limited sensitivity for soft tissue pathology and early-stage disease processes, and it cannot replace conventional autopsy in determining the COD in SUD cases. The value of PMCT in SUD investigations is not in directly diagnosing the COD, but in excluding alternative explanations, guiding targeted examinations, and providing supportive evidence. This integrative role makes PMCT a crucial component of modern forensic workflows, particularly in cases where the COD remains elusive after routine examination.
PMCTA
Postmortem computed tomography angiography (PMCTA) represents an important extension of PMCT, enabling detailed visualization of the vascular system through the administration of contrast agents. The primary contribution of PMCTA in SUD investigations is the detection and exclusion of vascular COD that may not be apparent on standard autopsy[198,199]. PMCTA allows for enhanced visualization of the coronary arteries and major vessels, facilitating the identification of stenosis, occlusion, or abnormal contrast distribution patterns[198,200-202]. Even when these findings are not definitive, they can help reclassify cases initially considered as SUD into more specific cardiovascular categories.
A limitation of PMCTA lies in the use of contrast agents, which can introduce artifacts such as extravasation or artificial vessel distension and may complicate interpretation. Additionally, postmortem changes in vascular tone and permeability can affect contrast distribution, potentially leading to false-positive or false-negative findings[198]. For this reason, the timing of PMCTA and the choice of contrast medium are critical factors in ensuring reliable results. PMCTA provides a valuable adjunct in the investigation of SUD by enhancing vascular assessment, facilitating the exclusion of occult vascular causes, and supporting targeted diagnostic strategies.
PMMRI
Postmortem magnetic resonance imaging (PMMRI) represents a critical advancement in virtual autopsy, particularly in the investigation of SUD, offering superior soft tissue contrast and provides unique insights into subtle pathological changes that may underlie functionally mediated deaths[203]. The most significant contribution of PMMRI in SUD lies in its ability to detect subtle myocardial abnormalities that are not readily identifiable through gross examination or even routine histology. In conditions such as ACM, early-stage myocardial changes may be unevenly distributed and easily missed during standard sampling[191,204]. PMMRI enables a more comprehensive, whole-heart assessment, allowing for the identification of regional signal alterations that may correspond to underlying pathological substrates. These findings can then guide targeted histological sampling and improve the diagnostic yield of subsequent analyses.
PMMRI provides substantial advantages in the assessment of the central nervous system. In cases involving brain softening, edema, or subtle hemorrhagic changes, PMMRI has demonstrated superior sensitivity compared to both PMCT and conventional autopsy[194,201], allowing for improved visualization of gray-white matter differentiation, detection of microhemorrhages, and characterization of liquefactive changes that may not be appreciable during dissection. These capabilities are particularly relevant in SUD cases where neurological causes, such as seizure-related death or central autonomic dysfunction, are suspected but remain difficult to confirm.
In addition, advanced MRI techniques, such as magnetic resonance spectroscopy (MRS), have been explored for postmortem biochemical analysis[205-208]. These approaches may offer insights into metabolic conditions or substance exposure prior to death. However, their current forensic applicability remains limited due to variability and insufficient accuracy, and they should be regarded as experimental rather than routine tools in SUD investigation.
ARTIFICIAL INTELLIGENCE IN SUDDEN UNEXPLAINED DEATH
Machine learning
ML has emerged as a particularly adaptable tool for handling complex and heterogeneous data[209]. Given its characteristic of allowing patterns to be learned directly from empirical observations, ML has been introduced in the COD identification in forensic practice, where the diagnostic process is often challenged by the absence of definitive structural findings at conventional autopsy[210]. In such cases, ML offers a framework capable of integrating diverse forms of evidence, thereby providing a more comprehensive basis for forensic interpretation.
From a methodological perspective, ML approaches can be broadly divided into supervised and unsupervised learning. Supervised learning involves training models on labeled datasets to perform tasks such as classification or regression, whereas unsupervised learning focuses on identifying intrinsic structures within unlabeled data, such as clustering or dimensionality reduction[211]. In SUD cases, the central issue is the gradual reduction of uncertainty through the integration of weak or indirect signals[210]. ML can detect patterns that are not immediately apparent through conventional statistical or visual analysis, thereby transforming fragmented observations into more coherent biological or forensic narratives.
One of the most mature areas for ML application in death and diseases is omics-based analysis[212]. Postmortem biological samples, such as cardiac blood, peripheral blood, or myocardial tissue, can yield high-dimensional datasets through multi-omics researches. In SUDs, metabolic disturbances - such as those associated with early ischemia, ion channel dysfunction, or systemic metabolic imbalance - tend to manifest as subtle, coordinated changes across multiple metabolites[213], where multivariate patterns can be captured by ML algorithms. For instance, supervised models such as random forest or SVM can be trained to distinguish SUD cases from controls by identifying combinations of metabolites that collectively contribute to classification[214]. In practical terms, ML-assisted metabolomics analysis can help forensic investigators move beyond descriptive findings toward more nuanced interpretations, such as the presence of metabolic signatures consistent with arrhythmogenic mechanisms or systemic physiological stress[123,215]. Although these findings may not be definitive on their own, they contribute to a cumulative evidentiary framework that supports COD assessment in otherwise unexplained cases.
A second major domain where ML demonstrates significant utility is molecular autopsy[216], particularly in the interpretation of genetic data. Advances in NGS have introduced a new challenge of identifying numerous VUS[217,218], many of which cannot be easily classified as pathogenic or benign using conventional criteria. More importantly, ML enables a shift from single-case interpretation to cohort-level analysis. By analyzing data across multiple SUD cases, unsupervised learning methods such as clustering can identify patterns of variant co-occurrence or shared genetic profiles. This is particularly valuable in conditions like channelopathies, where diagnosis relies heavily on molecular evidence. In addition, ML can facilitate the integration of genetic data with phenotypic and circumstantial information, such as age, sex, family history, and scene findings. This multi-layered approach reflects the reality of forensic practice, where conclusions are rarely based on a single line of evidence[217].
The application of ML to virtual autopsy represents a more recent but rapidly evolving area[219,220]. Postmortem imaging techniques, particularly PMCT and PMMRI, generate large volumes of data that are often underutilized due to the complexity of interpretation and the presence of postmortem artifacts[193,221]. In SUD cases, imaging findings are frequently subtle and nonspecific, which limits their standalone diagnostic value. ML can enhance the utility of these data by providing tools for pattern recognition and quantitative analysis[222]. For example, supervised learning models can be trained to identify imaging features associated with specific pathological conditions[205]. Moreover, ML-based approaches can provide consistent criteria for identifying and quantifying features, thereby avoiding the variability between observers[222].
A critical barrier to the widespread application of ML in forensic SUD investigation is the lack of large-scale, multi-center, standardized datasets. Unlike clinical medicine, where initiatives such as TCGA and UK Biobank have enabled data sharing across institutions, forensic genetics currently lacks comparable resources. Recently, a multi-center dataset comprising over 16 million high-resolution image patches, 2,228 vision-language pairs, and 471 distinct diagnostic outcomes from three premier forensic cohorts has been successfully compiled for AI model development[223]. This example underscores the potential of shared forensic data resources. Therefore, the establishment of multi-center shared datasets with standardized protocols for sample collection, sequencing, and data annotation is urgently needed to train robust ML models and enable cross-population validation.
However, data sharing in forensic genetics faces substantial privacy and legal barriers. Studies have shown that as few as 10 common SNPs are sufficient to identify individuals from a reference database of ~5,000 haplotypes, and 20-30 SNPs can identify first-order relatives, demonstrating that genetic data are inherently re-identifiable even when anonymized[224]. This raises serious questions about whether "de-identified" forensic DNA profiles can truly guarantee anonymity[225]. The legal basis for accessing genetic databases for research or investigative purposes remains ambiguous. Cross-border data sharing is further complicated by jurisdictional conflicts between divergent national privacy laws and a lack of harmonized international legal frameworks[226]. Jurisdictional conflicts arise from divergent national privacy laws, and concerns over function creep, where data collected for humanitarian purposes (e.g., missing persons identification) may be repurposed for law enforcement, have been raised by multiple stakeholders[226]. Furthermore, secondary use of biobank samples for forensic purposes without explicit consent remains under-regulated[225]. These challenges underscore the need for harmonized legal frameworks, transparent governance, and stakeholder engagement to enable responsible data sharing without compromising individual privacy rights.
The integration of ML into SUD investigation reflects a broader shift in forensic medicine from descriptive to data-driven analysis. ML serves as a complementary tool that enhances the interpretation of complex datasets. By bridging the gap between omics, molecular autopsy, and virtual autopsy, ML contributes to a more holistic understanding of SUD, ultimately supporting more informed and transparent forensic conclusions.
Deep learning
Deep learning (DL), as an advanced branch of ML, has introduced a fundamentally different approach to data analysis by enabling models to automatically learn hierarchical representations from raw input data[216]. Unlike traditional ML methods that rely on manually selected features, DL architectures - particularly convolutional neural networks (CNNs), recurrent neural networks (RNNs), and related variants - are capable of extracting complex, non-linear patterns directly from high-dimensional datasets[216].
DL improves data from molecular autopsy by modeling complex, nonlinear relationships across large-scale genomic datasets, functional annotations, and evolutionary features, thereby enhancing the accuracy and depth of pathogenicity prediction for both coding and non-coding variants. For instance, deleterious annotation of genetic variants using neural networks (DANN) has been developed employing a DL architecture trained on functional annotations similar to those used in combined annotation-dependent depletion (CADD), enabling improved discrimination between benign and pathogenic variants[227]. By capturing nonlinear interactions among diverse genomic features, such models provide probabilistic assessments of variant pathogenicity even in the absence of direct experimental evidence. In SUD cases, this is particularly valuable for prioritizing rare or novel variants that cannot be confidently classified using conventional guidelines such as those from the ACMG. Similarly, PrimateAI incorporates evolutionary information derived from primate genomes to evaluate the functional impact of missense variants[228], leveraging cross-species conservation to identify potentially deleterious substitutions. DeepSEA and Basenji utilize CNNs to predict chromatin accessibility, transcription factor binding, and gene expression directly from DNA sequences[229,230]. Additionally, PromoterAI further refines this approach by specifically predicting the impact of promoter variants[231], enhancing the resolution of regulatory variant interpretation. SpliceAI leverages deep CNNs to capture long-range dependencies within pre-mRNA sequences, enabling accurate prediction of splice site disruptions caused by genetic variants. This is particularly relevant in forensic cases, as certain variants previously classified as synonymous or benign may in fact exert pathogenic effects by altering RNA splicing[232,233]. In practice, these predictions can be integrated with RNA sequencing or in vitro functional assays to establish a more robust evidentiary basis.
DL has also shown immediate impact in virtual autopsy, particularly in the analysis of PMCT and PMMRI data. DL models can be trained to detect patterns associated with SUDs such as ACM, including diffuse fatty infiltration or subtle myocardial remodeling, which may not be apparent on routine visual inspection[222]. Another practical advantage of DL in virtual autopsy is its ability to enable quantitative and standardized analysis[219]. In SUD cases, where findings may be borderline or non-specific, such quantitative approaches can add an additional layer of evidence that supports or refines forensic conclusions.
Despite these promising applications, it is important to recognize that DL in SUD investigation remains at an early stage, and several challenges must be addressed before widespread adoption. One of the main limitations is the availability of high-quality, well-annotated datasets, which are essential for training reliable models. In forensic medicine, data are often limited in size and subject to variability in acquisition and documentation. In addition, the “black box” nature of many DL models raises concerns about interpretability, particularly in legal contexts where transparency and reproducibility are critical. For this reason, there is increasing interest in developing explainable DL approaches that provide insight into how predictions are made, thereby enhancing trust and usability in forensic applications. By enabling the analysis of complex, high-dimensional data in a more integrated and automated manner, DL supports a shift toward more data-driven and system-level interpretations of SUD. When combined with traditional forensic methods, it has the potential to improve diagnostic yield, reduce uncertainty, and provide a more comprehensive understanding of cases that would otherwise remain unexplained [Figure 4].
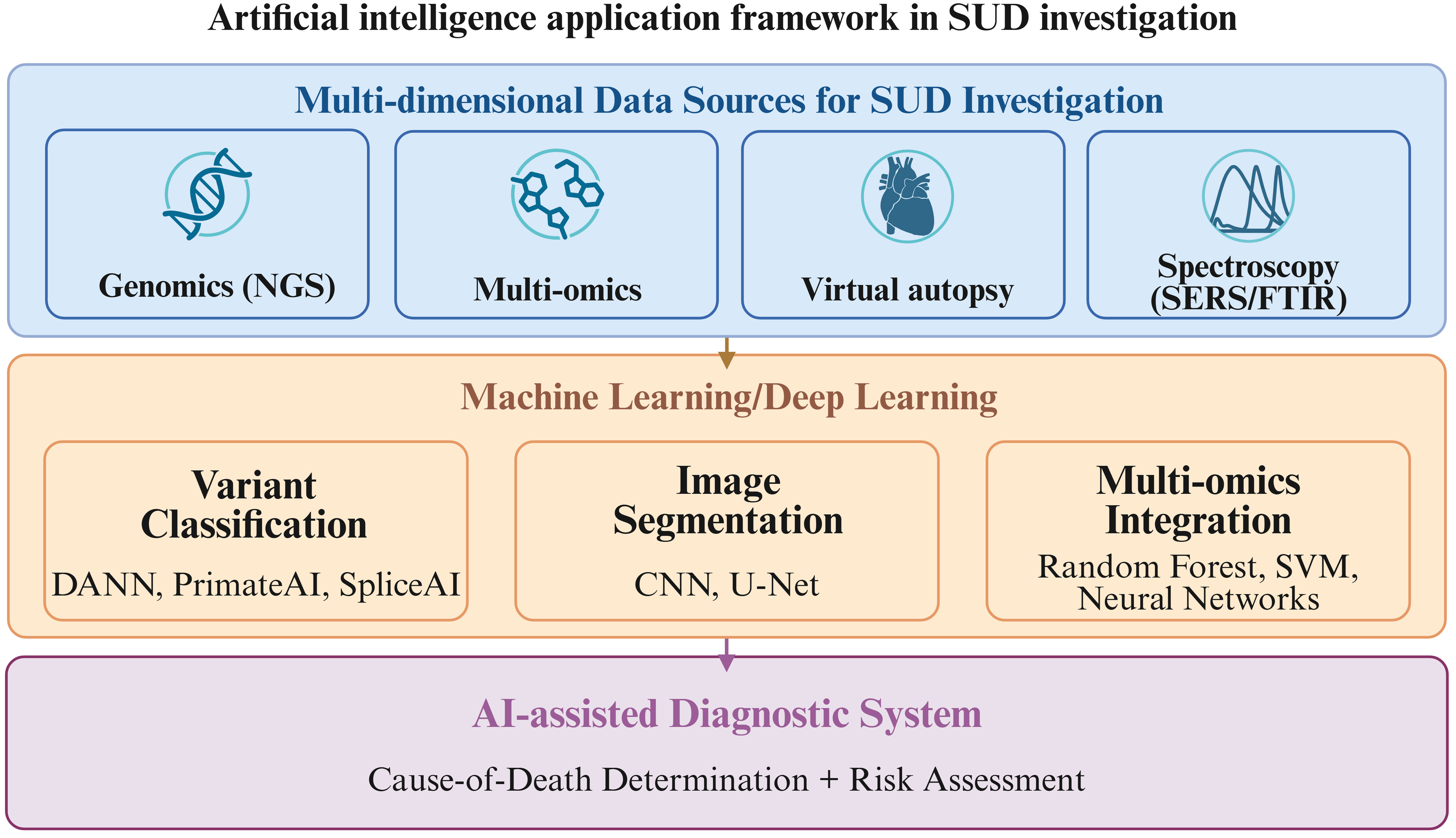
Figure 4. Integrated analytical framework for the application of AI in forensic investigation of SUDs. This schematic illustrates the multi-modal strategy combining multi-omics and spectroscopic approaches, virtual autopsy imaging techniques, and AI (ML and DL) for precise COD determination, pathophysiological mechanism interpretation, and evidence-based diagnosis in SUD cases (including SCD, SIDS, and SUDEP). Created in BioRender. qi, M. (2026) https://BioRender.com/oepjqkf. SUD: Sudden unexplained death; NGS: next-generation sequencing; SERS: surface-enhanced Raman spectroscopy; FTIR: Fourier transform infrared; DANN: deleterious annotation of genetic variants using neural networks; CNN: convolutional neural network; SVM: support vector machine; AI: artificial intelligence.
CONCLUSION
The trajectory of forensic medicine is increasingly defined by its capacity to integrate knowledge and technologies from diverse scientific domains. The conventional boundaries between forensic sub-disciplines and external fields such as clinical medicine, biology, engineering, and the humanities are becoming progressively more permeable. This interdisciplinary convergence is not merely an option but a necessity for addressing the growing complexity of forensic casework in the information-driven and intelligent era.
This review provides references and advice for the postmortem investigation of decedents with SUD for forensic pathologists, highlighting recent technical innovations including molecular autopsy, multi-omics approaches (proteomics, metabolomics, transcriptomics, and spectroscopic techniques such as Raman and FTIR), virtual autopsy (PMCT, PMCTA, and PMMRI), and the application of AI that are progressively transforming SUD investigation. These advanced methods enable high-throughput genetic screening, functional characterization of antemortem biochemical states, non-invasive detection of subtle pathological changes, and enhanced interpretation of complex, high-dimensional data. Despite their considerable potential to improve COD determination and facilitate cascade screening in affected families, none of these techniques have yet been incorporated into routine postmortem diagnostic criteria, particularly in China.
Despite the considerable promise of these advanced techniques, their integration into routine forensic practice, particularly in China, faces multiple practical hurdles. To bridge the gap between innovation and implementation, systematic efforts are required in four key domains.
First, dedicated funding and infrastructure development are essential to equip forensic institutions with NGS platforms, mass spectrometers, postmortem CT/MRI scanners, and the computational resources needed for AI-based analysis. Multi-center collaborations should be financially supported to establish shared databases that enable robust validation of molecular and imaging biomarkers.
Second, workforce training and interdisciplinary education must be prioritized. Forensic pathologists and technicians need specialized training programs in molecular genetics, bioinformatics, multi-omics data interpretation, and AI-assisted diagnostics. Cross-disciplinary curricula involving forensic medicine, clinical genetics, and computational biology should be developed at both undergraduate and postgraduate levels.
Third, legal and ethical frameworks urgently require updating to accommodate these technological advances. National guidelines are needed to govern the use of postmortem genetic testing, including protocols for sample collection, variant interpretation (following ACMG/AMP standards), reporting of incidental findings, and cascade screening of at-risk relatives. Legislation must also address data privacy protection, informed consent for genetic analysis in deceased individuals, and the ethical boundaries of AI-assisted cause-of-death determination.
Fourth, standardization and accreditation systems should be established to ensure quality control and legal admissibility of evidence generated by these techniques. Unified technical protocols for molecular autopsy (e.g., panel design, bioinformatics pipelines, VUS reclassification intervals), virtual autopsy imaging acquisition, and multi-omics biomarker validation are needed. Accreditation programs for forensic laboratories implementing these methods would enhance reliability and court acceptance.
Without these complementary investments in infrastructure, training, law, and quality assurance, the transformative potential of molecular autopsy, multi-omics, virtual imaging, and AI will remain largely unrealized in routine forensic casework. Nevertheless, conventional macroscopic and histopathological examination remains the indispensable gold standard against which all ancillary techniques must be validated. A strategic, multi-stakeholder roadmap is urgently needed to translate scientific innovation into tangible improvements in SUD investigation and, ultimately, to reduce the proportion of unexplained deaths and prevent additional fatalities in affected families.
Future research should prioritize the validation of novel biomarkers, establishment of standardized protocols, and development of interpretable AI models to fully integrate these complementary approaches into forensic practice, ultimately reducing the proportion of unexplained deaths and advancing precision forensic medicine. Here, we provided our suggested integrated workflow for the forensic investigation of SUD [Figure 5]. Further studies are required to develop novel indicators and techniques for forensic application. Nevertheless, conventional macroscopic and histopathological examination remains the indispensable gold standard against which all ancillary techniques must be validated.
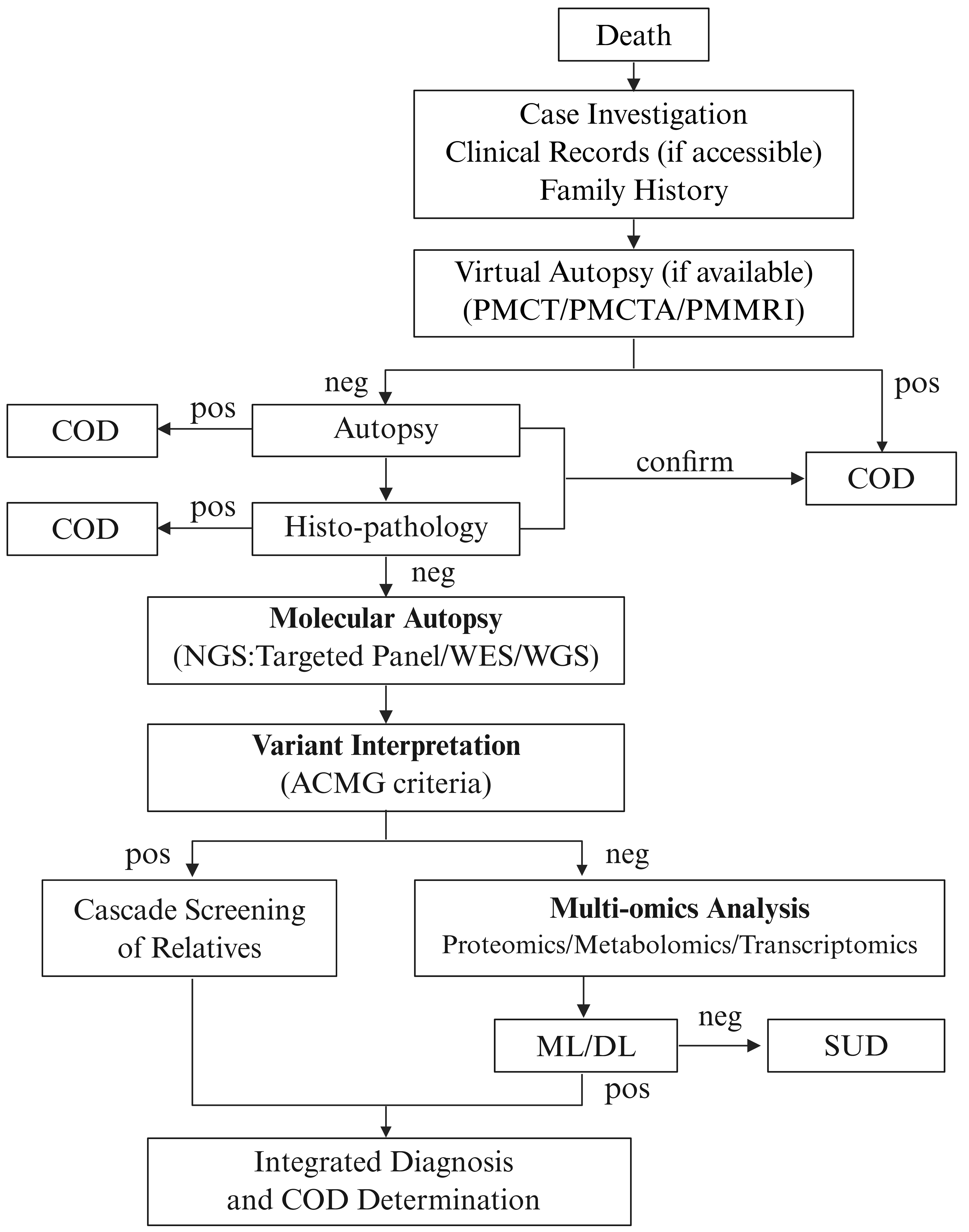
Figure 5. Integrated workflow for the forensic investigation of SUD. The diagram illustrates a stepwise approach beginning with virtual autopsy, followed by conventional autopsy and molecular autopsy using NGS technologies. Positive genetic findings undergo variant interpretation according to ACMG guidelines, enabling cascade screening of at-risk relatives. Cases with negative or uncertain results proceed to multi-omics analysis (proteomics, metabolomics, transcriptomics) with AI-assisted integration for comprehensive diagnosis. Created in BioRender. qi, M. (2026) https://BioRender.com/jvfuzo6. COD: Cause of death; PMCT: postmortem computed tomography; PMCTA: postmortem computed tomography angiography; PMMRI: postmortem magnetic resonance imaging; NGS: next-generation sequencing; WES: whole-exome sequencing; WGS: whole-genome sequencing; ACMG: American College of Medical Genetics and Genomics; ML: machine learning; DL: deep learning; SUD: sudden unexplained death; AI: artificial intelligence.
In conclusion, the future of forensic medicine lies in proactive, multidisciplinary collaboration. By embracing innovation while upholding scientific rigor and ethical responsibility, the forensic community can generate original knowledge, improve evidentiary reliability, and better serve the evolving needs of the judicial system. The path forward requires not only technological advancement but also a sustained commitment to cross-disciplinary education, open science, and international partnership.
DECLARATIONS
Acknowledgments
The graphical abstract was created in BioRender. qi, M. (2026) https://BioRender.com/28n6jrq.
Authors’ contributions
Drafted the manuscript: Yu Y, Zhu J, Han X, Peng X, Cao Y (Yongjie Cao), Wang F
Prepared figures and tables: Meng Q, Qu D, Sheng M
Reviewed and edited the manuscript: Chen F, Cao Y (Yue Cao), Wang K
All authors have read and approved the final version of the manuscript.
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tools DeepSeek (version 3.2, released 2025-12) and Kimi (version 2.6, released 2026-4-20) were used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This work was supported by grants from the National Natural Science Foundation of China (82225023).
Conflicts of interest
Chen F is an Editorial Board Member of Legal Medicine Research. Chen F was not involved in any aspect of the editorial process for this manuscript, including reviewer selection, manuscript handling, and decision-making. The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of Patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015;36:2793-867.
2. Behr E, Wood D, Wright M, et al. Cardiological assessment of first-degree relatives in sudden arrhythmic death syndrome. The Lancet. 2003;362:1457-9.
3. Raju H, Behr ER. Unexplained sudden death, focussing on genetics and family phenotyping. Curr Opin Cardiol. 2013;28:19-25.
4. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018;138.
5. Wu Q, Zhang L, Zheng J, et al. Forensic pathological study of 1656 cases of sudden cardiac death in southern China. Medicine (Baltimore). 2016;95:e2707.
6. Hua W, Zhang L, Wu Y, et al. Incidence of sudden cardiac death in China. J Am Coll Cardiol. 2009;54:1110-8.
7. Basso C, Aguilera B, Banner J, et al. ; on behalf of the Association for European Cardiovascular Pathology. Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows Arch. 2017;471:691-705.
8. Holm PH, Jensen THL, Westaby J, et al. quantitative histological insights into sudden arrhythmic death syndrome: findings from a forensic autopsy cohort. APMIS. 2026;134:e70169.
9. Fialho GL, Wolf P, Walz R, Lin K. SUDEP - more attention to the heart? A narrative review on molecular autopsy in epilepsy. Seizure. 2021;87:103-6.
10. Stiles MK, Wilde AA, Abrams DJ, et al. 2020 APHRS/HRS expert consensus statement on the investigation of decedents with sudden unexplained death and patients with sudden cardiac arrest, and of their families. Heart Rhythm. 2021;18:e1-e50.
11. Tseng ZH, Olgin JE, Vittinghoff E, et al. Prospective countywide surveillance and autopsy characterization of sudden cardiac death: POST SCD study. Circulation. 2018;137:2689-700.
12. Pouleur A, Barkoudah E, Uno H, et al. Pathogenesis of sudden unexpected death in a clinical trial of patients with myocardial infarction and left ventricular dysfunction, heart failure, or both. Circulation. 2010;122:597-602.
14. Barranco R, Caristo I, Molinelli A, Rocca G, Vernazza N, Ventura F. Update on the similarities between SADS, SIDS, and SUDEP: three sides of the same pyramid? Int J Legal Med. 2025;140:1-12.
15. Lou J, Chen H, Huang S, Chen P, Yu Y, Chen F. Update on risk factors and biomarkers of sudden unexplained cardiac death. J Forensic Leg Med. 2022;87:102332.
16. Huang S, Chen J, Song M, et al. Whole-exome sequencing and electrophysiological study reveal a novel loss-of-function mutation of KCNA10 in epinephrine provoked long QT syndrome with familial history of sudden cardiac death. Leg Med. 2023;62:102245.
17. Sheng M, Zheng H, Zhang L, et al. SCN5A c.4720G> A: a rare genetic variant associated with familial sick sinus syndrome and sudden cardiac death. Int J Legal Med. 2026;140:1951-62.
18. Huang S, Zhang J, Wan H, et al. Plasma extracellular vesicles microRNA-208b-3p and microRNA-143-3p as novel biomarkers for sudden cardiac death prediction in acute coronary syndrome. Molecular Omics. 2023;19:262-73.
19. Lou J, Cao Y, Yu Y, et al. Investigation of heart lipid changes in acute β-AR activation-induced sudden cardiac death by time-of-flight secondary ion mass spectrometry. Analyst. 2020;145:5889-96.
20. Wan H, Huang S, Duan J, et al. Endogenous pyruvate and lactic dehydrogenase B in plasma extracellular vehicles predict sudden cardiac death risk in acute coronary syndrome: A multiomics study. Asian Heart J. 2026;2:14-25.
21. Femia G, Langlois N, Raleigh J, et al. Comparison of conventional autopsy with post-mortem magnetic resonance, computed tomography in determining the cause of unexplained death. Forensic Sci Med Pathol. 2021;17:10-8.
22. Solomon N, Gascho D, Adolphi NL, et al. The evolution of postmortem investigation: a historical perspective on autopsy's decline and imaging’s role in its revival. Front Radiol. 2025;5:1565012.
23. Tortosa Lopez JM. Histopathology in medico-legal autopsies: clinical foundation, legal mandate, and judicial guarantee. J Forensic Leg Med. 2025;115:102974.
24. Eckart RE, Shry EA, Burke AP, et al. Sudden death in young adults. J Am Coll Cardiol. 2011;58:1254-61.
25. Garcia-Elias A, Benito B. Ion channel disorders and sudden cardiac death. Int J Mol Sci. 2018;19:692.
26. Sieira J, Dendramis G, Brugada P. Pathogenesis and management of Brugada syndrome. Nat Rev Cardiol. 2016;13:744-56.
27. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease. J Am Coll Cardiol. 2019;73:e81-e192.
28. Chinese Society of Pathology, Chinese Medical Association Cardiovascular Disease Group of the Chinese Society of Pathology, Chinese Medical Association, et al. Chinese expert consensus statement on the autopsy and molecular diagnosis of sudden cardiac death. Chin Circ J. 2022;37:865-75.
29. Campuzano O, Tirón C, Martínez-barrios E, et al. The role of molecular autopsy in concealed cardiomyopathies. Genes. 2025;16:1273.
30. Isbister JC, Nowak N, Butters A, et al. “Concealed cardiomyopathy” as a cause of previously unexplained sudden cardiac arrest. Int J Cardiol. 2021;324:96-101.
31. Isbister JC, Nowak N, Yeates L, et al. Concealed cardiomyopathy in autopsy-inconclusive cases of sudden cardiac death and implications for families. J Am Coll Cardiol. 2022;80:2057-68.
32. Coll M, Alcalde M, Fernández-Falgueras A, et al. Value of molecular autopsy in suspected sudden cardiac death in the young. J Mol Diagn. 2025;27:859-68.
33. Delpire B, Dilling-Boer D, Ghekiere O, et al. Electroanatomical mapping may identify concealed arrhythmogenic cardiomyopathy in endurance athletes with complex ventricular arrhythmias. JACC: Case Reports. 2026;31:107493.
34. Tu E, Bagnall RD, Duflou J, Semsarian C. Post-mortem review and genetic analysis of sudden unexpected death in epilepsy (SUDEP) Cases. Brain Pathol. 2010;21:201-8.
35. Ruthirago D, Julayanont P, Karukote A, Shehabeldin M, Nugent K. Sudden unexpected death in epilepsy: ongoing challenges in finding mechanisms and prevention. Int J Neurosci. 2018;128:1052-60.
36. Farrell EK, Tang S, Feng H. Vanillin suppresses seizure-induced mortality in the DBA/1 mouse model of SUDEP. Neurosci Lett. 2026;877:138575.
37. Ryvlin P, Rheims S. SUDEP update 2026: recent advances in experimental and clinical research. Curr Opin Neurol. 2026;39:123-30.
38. Parisi P, Oliva A, Coll Vidal M, et al. Coexistence of epilepsy and Brugada syndrome in a family with SCN5A mutation. Epilepsy Res. 2013;105:415-8.
39. Bagnall RD, Crompton DE, Semsarian C. Genetic basis of sudden unexpected death in epilepsy. Front Neurol. 2017;8:348.
40. Chahal CAA, Tester DJ, Fayyaz AU, et al. Confirmation of cause of death via comprehensive autopsy and whole exome molecular sequencing in people with epilepsy and sudden unexpected death. JAHA. 2021;10:e021170.
41. Bagnall RD, Perucca P. ; for the ILAE Genetics Commission. ILAE genetic literacy series: postmortem genetic testing in sudden unexpected death in epilepsy. Epileptic Disord. 2023;25:472-9.
42. Brunklaus A, Feng T, Brünger T, et al. Gene variant effects across sodium channelopathies predict function and guide precision therapy. Brain. 2022;145:4275-86.
43. TASK FORCE ON SUDDEN INFANT DEATH SYNDROME. SIDS and Other sleep-related infant deaths: updated 2016 recommendations for a safe infant sleeping environment. Pediatrics. 2016;138:e20162938.
44. Goldstein RD, Blair PS, Sens MA, et al. ; The 3rd International Congress on Sudden Infant and Child Death. Inconsistent classification of unexplained sudden deaths in infants and children hinders surveillance, prevention and research: recommendations from The 3rd International Congress on Sudden Infant and Child Death. Forensic Sci Med Pathol. 2019;15:622-8.
45. Hakanen E, Oura P, Vauhkonen PK. Neuropathologic findings and age-related differences in Finnish pediatric medico-legal autopsies. J Forensic Sci. 2026;71:1246-54.
46. Kaler J, Hussain A, Lee S. Manifestation and pathogenesis of sudden infant death syndrome: a review. Crit Rev Eukaryot Gene Expr. 2020;30:111-20.
47. Bechtel K, Vincent GA, Sullivan B, Gaither J. Analysis of first and second sleep environments in unexplained sudden deaths in infants based on scene reenactment data. Am J Forensic Med Pathol. 2026;47:113-6.
48. Shapiro-Mendoza CK, Palusci VJ, Hoffman B, et al. ; AAP TASK FORCE ON SUDDEN INFANT DEATH SYNDROME, COUNCIL ON CHILD ABUSE AND NEGLECT, COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION, SECTION ON CHILD DEATH REVIEW AND PREVENTION, NATIONAL ASSOCIATION OF MEDICAL EXAMINERS. Half century since SIDS: a reappraisal of terminology. Pediatrics. 2021;148:e2021053746.
49. Cazzato F, Coll M, Grassi S, et al. Investigating cardiac genetic background in sudden infant death syndrome (SIDS). Int J Legal Med. 2024;138:2229-37.
50. Argentiero G, Talamo M, Amirante F, Cecchetto G, Solarino B. Effects of decomposition on the cardiovascular system: a systematic review. Forensic Sci Int. 2025;373:112529.
51. Byard RW. Artefacts due to putrefactive gas production - an overview. Med Sci Law. 2024;65:65-70.
52. Van Den Bogaert W, Alders L, Wuestenbergs J, Dequeker E, Van De Voorde W. Defining, exploring the sources and expressing post-mortem diagnostic uncertainty. Forensic Sci Med Pathol. 2024;21:728-35.
53. Martínez-Barrios E, Grassi S, Brión M, et al. Molecular autopsy: twenty years of post-mortem diagnosis in sudden cardiac death. Front Med. 2023;10:1118585.
54. Goodwin S, Mcpherson JD, Mccombie WR. Coming of age: ten years of next-generation sequencing technologies. Nat Rev Genet. 2016;17:333-51.
55. Castiglione V, Modena M, Aimo A, et al. Molecular autopsy of sudden cardiac death in the genomics era. Diagnostics. 2021;11:1378.
56. Salfati EL, Spencer EG, Topol SE, et al. Re-analysis of whole-exome sequencing data uncovers novel diagnostic variants and improves molecular diagnostic yields for sudden death and idiopathic diseases. Genome Med. 2019;11:83.
57. Semsarian C, Ingles J, Wilde AAM. Sudden cardiac death in the young: the molecular autopsy and a practical approach to surviving relatives. Eur Heart J. 2015;36:1290-6.
58. Ackerman MJ, Priori SG, Willems S, et al. HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies. Heart Rhythm. 2011;8:1308-39.
59. Baudhuin LM, Lagerstedt SA, Klee EW, Fadra N, Oglesbee D, Ferber MJ. Confirming variants in next-generation sequencing panel testing by sanger sequencing. J Mol Diagn. 2015;17:456-61.
60. Adams DR, Eng CM. Next-generation sequencing to diagnose suspected genetic disorders. N Engl J Med. 2018;379:1353-62.
61. Shamseldin HE, Alabdi L, Maddirevula S, et al. ; Molecular Autopsy Consortium. Lethal variants in humans: lessons learned from a large molecular autopsy cohort. Genome Med. 2021;13:161.
62. Osouf J, Schalk A, Schaefer E, et al. Genetic testing after sudden death with negative ancillary investigations: a French prospective study with multidisciplinary collaboration. Forensic Sci Int Genet. 2026;81:103375.
63. Federici G, Soddu S. Variants of uncertain significance in the era of high-throughput genome sequencing: a lesson from breast and ovary cancers. J Exp Clin Cancer Res. 2020;39:46.
65. Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17:405-24.
66. Biesecker LG, Harrison SM. The ACMG/AMP reputable source criteria for the interpretation of sequence variants. Genet Med. 2018;20:1687-8.
67. Caroselli S, Corona G, Fabiani M, et al. Reclassification of VUS Using ACMG/AMP criteria adapted for sarcomeric genes related to hypertrophic cardiomyopathy: resolution rate and considerations. Hum Mutat. 2025;2025:6500093.
68. Neves R, Tester DJ, Simpson MA, Behr ER, Ackerman MJ, Giudicessi JR. Exome sequencing highlights a potential role for concealed cardiomyopathies in youthful sudden cardiac death. Circ-Genom Precis Me. 2022;15:e003497.
69. Girolami F, Spinelli V, Maurizi N, et al. Genetic characterization of juvenile sudden cardiac arrest and death in Tuscany: the ToRSADE registry. Front Cardiovasc Med. 2022;9:1080608.
70. Scheiper-Welling S, Tabunscik M, Gross TE, et al. Variant interpretation in molecular autopsy: a useful dilemma. Int J Legal Med. 2022;136:475-82.
71. Doldi F, Willy K, Wolfes J, et al. Changing antiarrhythmic drug regimen in patients with amiodarone and ablation refractory ventricular tachyarrhythmias is associated with increased implantable cardioverter defibrillator shocks - a retrospective analysis from a large tertiary center. JCM. 2025;14:2859.
72. Strande NT, Riggs ER, Buchanan AH, et al. Evaluating the Clinical Validity of Gene-Disease Associations: an evidence-based framework developed by the clinical genome resource. Am J Hum Genet. 2017;100:895-906.
73. Rehm HL, Berg JS, Brooks LD, et al. ClinGen - the clinical genome resource. N Engl J Med. 2015;372:2235-42.
74. Hosseini SM, Kim R, Udupa S, et al. ; On behalf of the National Institutes of Health Clinical Genome Resource Consortium. Reappraisal of reported genes for sudden arrhythmic death: evidence-based evaluation of gene validity for Brugada syndrome. Circulation. 2018;138:1195-205.
75. Adler A, Novelli V, Amin AS, et al. An international, multicentered, evidence-based reappraisal of genes reported to cause congenital long QT syndrome. Circulation. 2020;141:418-28.
76. Walsh R, Adler A, Amin AS, et al. Evaluation of gene validity for CPVT and short QT syndrome in sudden arrhythmic death. Eur Heart J. 2022;43:1500-10.
77. James CA, Jongbloed JD, Hershberger RE, et al. International evidence based reappraisal of genes associated with arrhythmogenic right ventricular cardiomyopathy using the clinical genome resource framework. Circ-Genom Precis Me. 2021;14:e003273.
78. Ingles J, Goldstein J, Thaxton C, et al. Evaluating the clinical validity of hypertrophic cardiomyopathy genes. Circ-Genom Precis Me. 2019;12:e002460.
79. Hespe S, Waddell A, Asatryan B, et al. Genes associated with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2025;85:727-40.
80. Jordan E, Peterson L, Ai T, et al. Evidence-based assessment of genes in dilated cardiomyopathy. Circulation. 2021;144:7-19.
81. Tsuji-Wakisaka K, Akao M, Ishii TM, et al. Identification and functional characterization of KCNQ1 mutations around the exon 7-intron 7 junction affecting the splicing process. Biochim Biophys Acta Mol Basis Dis. 2011;1812:1452-9.
82. Kanters JK, Larsen LA, Orholm M, et al. Novel donor splice site mutation in the KVLQT1 gene is associated with long QT syndrome. J Cardiovasc Electrophysiol. 2007;9:620-4.
83. Piippo K, Swan H, Pasternack M, et al. A founder mutation of the potassium channel KCNQ1 in long QT syndrome. J Am Coll Cardiol. 2001;37:562-8.
84. Aromolaran AS, Subramanyam P, Chang DD, Kobertz WR, Colecraft HM. LQT1 mutations in KCNQ1 C-terminus assembly domain suppress IKs using different mechanisms. Cardiovasc Res. 2014;104:501-11.
85. Zhang Y, Zhou N, Jiang W, et al. A missense mutation (G604S) in the S5/pore region of HERG causes long QT syndrome in a Chinese family with a high incidence of sudden unexpected death. Eur J Pediatr. 2006;166:927-33.
86. Huo J, Zhang Y, Huang N, et al. The G604S-hERG mutation alters the biophysical properties and exerts a dominant-negative effect on expression of hERG channels in HEK293 cells. Pflugers Arch - Eur J Physiol. 2008;456:917-28.
87. Sanguinetti MC, Curran ME, Spector PS, Keating MT. Spectrum of HERG K+-channel dysfunction in an inherited cardiac arrhythmia. Proc Natl Acad Sci USA. 1996;93:2208-12.
88. Crimmins S, Vashit S, Doyle L, Harman C, Turan O, Turan S. A multidisciplinary approach to prenatal treatment of congenital long QT syndrome. J Clin Ultrasound. 2016;45:168-70.
89. Zarraga IG, Zhang L, Stump MR, Gong Q, Vincent GM, Zhou Z. Nonsense-mediated mRNA decay caused by a frameshift mutation in a large kindred of type 2 long QT syndrome. Heart Rhythm. 2011;8:1200-6.
90. Hu D, Li Y, Zhang J, et al. The phenotypic spectrum of a mutation hotspot responsible for the short QT Syndrome. JACC Clin Electrophysiol. 2017;3:727-43.
91. Sun Y, Quan X, Fromme S, et al. A novel mutation in the KCNH2 gene associated with short QT syndrome. J Mol Cell Cardiol. 2011;50:433-41.
92. Corona-Rivera JR, Barrios-Prieto E, Nieto-García R, et al. Unusual retrospective prenatal findings in a male newborn with Timothy syndrome type 1. Eur J Med Genet. 2015;58:332-5.
93. Splawski I, Timothy KW, Sharpe LM, et al. CaV1.2 calcium channel dysfunction causes a multisystem disorder including arrhythmia and autism. Cell. 2004;119:19-31.
94. Santos LF, Rodrigues B, Moreira D, et al. Criteria to predict carriers of a novel SCN5A mutation in a large Portuguese family affected by the Brugada syndrome. Europace. 2012;14:882-8.
95. Selga E, Campuzano O, Pinsach-Abuin M, et al. Comprehensive genetic characterization of a Spanish Brugada syndrome cohort. PLoS ONE. 2015;10:e0132888.
96. Probst V, Wilde AA, Barc J, et al. SCN5A mutations and the role of genetic background in the pathophysiology of Brugada syndrome. Circ Cardiovasc Genet. 2009;2:552-7.
97. Keller D, Rougier J, Kucera J, et al. Brugada syndrome and fever: genetic and molecular characterization of patients carrying mutations. Cardiovasc Res. 2005;67:510-9.
98. Makita N, Behr E, Shimizu W, et al. The E1784K mutation in SCN5A is associated with mixed clinical phenotype of type 3 long QT syndrome. J Clin Investig. 2008:JCI34057.
99. Okata S, Yuasa S, Suzuki T, et al. Embryonic type Na+ channel β-subunit, SCN3B masks the disease phenotype of Brugada syndrome. Sci Rep. 2016;6:34198.
100. Josephs K, Patel K, Janson CM, Montagna C, Mcdonald TV. Compound heterozygous CASQ2 mutations and long-term course of catecholaminergic polymorphic ventricular tachycardia. Mol Genet Genomic Med. 2017;5:788-94.
101. Li Q, Guo R, Gao L, et al. CASQ2 variants in Chinese children with catecholaminergic polymorphic ventricular tachycardia. Mol Genet Genomic Med. 2019;7:e949.
102. Lahat H, Pras E, Eldar M. A missense mutation in CASQ2 is associated with autosomal recessive catecholamine-induced polymorphic ventricular tachycardia in Bedouin families from Israel. Ann Med. 2009;36:87-91.
103. Dirksen W, Lacombe V, Chi M, et al. A mutation in calsequestrin, CASQ2D307H, impairs sarcoplasmic reticulum Ca2+ handling and causes complex ventricular arrhythmias in mice. Cardiovasc Res. 2007;75:69-78.
104. Shimamoto K, Sumitomo N, Nabeshima T, et al. Novel compound heterozygous variants in trans-2,3-enoyl-coenzyme a reductase-like gene associated with catecholaminergic polymorphic ventricular tachycardia. JACC: Case Reports. 2024;29:102364.
105. Bailey C, Blair E, Garratt C, Newman WG. Effective cascade screening through identification of a mutation in RYR2 in a large family with a history of sudden death. J Cardiol Cases. 2016;13:9-13.
106. Arad M, Glikson M, El-Ani D, Monserrat-Inglesias L. A family with recurrent sudden death and no clinical clue. Ann Noninvasive Electrocardiol. 2012;17:387-93.
107. Rabbani B, Khorgami M, Dalili M, Zamani N, Mahdieh N, Gollob MH. Novel cases of pediatric sudden cardiac death secondary to TRDN mutations presenting as long QT syndrome at rest and catecholaminergic polymorphic ventricular tachycardia during exercise: The TRDN arrhythmia syndrome. Am J Med Genet A. 2021;185:3433-45.
108. Al-Hassnan ZN, Al-Fayyadh M, Al-Ghamdi B, et al. Clinical profile and mutation spectrum of long QT syndrome in Saudi Arabia: the impact of consanguinity. Heart Rhythm. 2017;14:1191-9.
109. Vanoye CG, Desai RR, Fabre KL, et al. High-throughput functional evaluation ofKCNQ1 decrypts variants of unknown significance. Circ-Genom Precis Me. 2018;11:e002345.
110. Roberts JD, Krahn AD, Ackerman MJ, et al. Loss-of-function KCNE2 variants: true monogenic culprits of long-QT syndrome or proarrhythmic variants requiring secondary provocation? Circ-Arrhythmia Elec. 2017;10:e005282.
111. Bains S, Dotzler SM, Krijger C, et al. A phenotype-enhanced variant classification framework to decrease the burden of missense variants of uncertain significance in type 1 long QT syndrome. Heart Rhythm. 2022;19:435-42.
112. Brewer KR, Vanoye CG, Huang H, et al. Integrative analysis of KCNQ1 variants reveals molecular mechanisms of type 1 long QT syndrome pathogenesis. Proc Natl Acad. Sci USA. 2025;122:e2412971122.
113. Barsheshet A, Goldenberg I, O-Uchi J, et al. Mutations in cytoplasmic loops of the KCNQ1 channel and the risk of life-threatening events: implications for mutation-specific response to β-blocker therapy in type 1 long-QT syndrome. Circulation. 2012;125:1988-96.
114. Wang Z, Tristani-Firouzi M, Xu Q, Lin M, Keating M, Sanguinetti M. Functional effects of mutations in KvLQT1 that cause long QT syndrome. J Cardiovasc Electrophysiol. 2007;10:817-26.
115. Giudicessi JR, Ackerman MJ. Prevalence and potential genetic determinants of sensorineural deafness in KCNQ1 homozygosity and compound heterozygosity. Circ Cardiovasc Genet. 2013;6:193-200.
116. Westphal DS, Burkard T, Moscu-Gregor A, Gebauer R, Hessling G, Wolf CM. Reclassification of genetic variants in children with long QT syndrome. Mol Genet Genomic Med. 2020;8:e1300.
117. Mak CM, Chen SP, Mok N, et al. ; Chemical Pathology Laboratory, Kowloon West Cluster Laboratory Genetic Service, Department of Pathology, Princess Margaret Hospital, Laichikok, Hong Kong. Genetic basis of channelopathies and cardiomyopathies in Hong Kong Chinese patients: a 10-year regional laboratory experience. Hong Kong Med J. 2018.
118. Koponen M, Marjamaa A, Hiippala A, et al. Follow-up of 316 molecularly defined pediatric long-qt syndrome patients: clinical course, treatments, and side effects. Circ-Arrhythmia Elec. 2015;8:815-23.
119. Ackerman MJ, Tester DJ, Porter CJ. Swimming, a gene-specific arrhythmogenic trigger for inherited long QT syndrome. Mayo Clin Proc. 1999;74:1088-94.
120. Cuneo BF, Etheridge SP, Horigome H, et al. Arrhythmia phenotype during fetal life suggests long-QT syndrome genotype: risk stratification of perinatal long-QT syndrome. Circ-Arrhythmia Elec. 2013;6:946-51.
121. Jons C, O-Uchi J, Moss AJ, et al. Use of mutant-specific ion channel characteristics for risk stratification of long QT syndrome patients. Sci Transl Med. 2011;3.
122. Bianchi L, Priori SG, Napolitano C, et al. Mechanisms of I(Ks) suppression in LQT1 mutants. Am J Physiol-Heart C. 2000;279:H3003-11.
123. Sacco MA, Mastrangelo H, Neri G, Aquila I. Post-mortem biomarkers in sudden cardiac death: from classical biochemistry to molecular autopsy and multi-omics forensic approaches. Int J Mol Sci. 2026;27:670.
124. Krasny L, Bland P, Kogata N, et al. SWATH mass spectrometry as a tool for quantitative profiling of the matrisome. J Proteomics. 2018;189:11-22.
125. Gillet LC, Navarro P, Tate S, et al. Targeted data extraction of the MS/MS spectra generated by data-independent acquisition: a new concept for consistent and accurate proteome analysis. Mol Cell Proteomics. 2012;11:O111.016717.
126. Chantada-Vázquez MDP, Bravo SB, Barbosa-Gouveia S, Alvarez JV, Couce ML. Proteomics in inherited metabolic disorders. Int J Mol Sci. 2022;23:14744.
127. Elmiger MP, Poetzsch M, Steuer AE, Kraemer T. Assessment of simpler calibration models in the development and validation of a fast postmortem multi-analyte LC-QTOF quantitation method in whole blood with simultaneous screening capabilities using SWATH acquisition. Anal Bioanal Chem. 2017;409:6495-508.
128. Sacco MA, Gualtieri S, Grimaldi G, et al. The role of cardiac troponins in postmortem diagnosis of myocardial ischemia: a systematic review. Int J Mol Sci. 2024;26:105.
129. Aydin S, Ugur K, Aydin S, Sahin İ, Yardim M. Biomarkers in acute myocardial infarction: current perspectives. Vasc Health Risk Manag..
130. Netala VR, Hou T, Wang Y, Zhang Z, Teertam SK. Cardiovascular biomarkers: tools for precision diagnosis and prognosis. Int J Mol Sci. 2025;26:3218.
131. Ghormade PS, Kumar NB, Tingne CV, Keoliya AN. Distribution & diagnostic efficacy of cardiac markers CK-MB & LDH in pericardial fluid for postmortem diagnosis of ischemic heart disease. J Forensic Leg Med. 2014;28:42-6.
132. Chen J, Inamori-Kawamoto O, Michiue T, Ikeda S, Ishikawa T, Maeda H. Cardiac biomarkers in blood, and pericardial and cerebrospinal fluids of forensic autopsy cases: a reassessment with special regard to postmortem interval. Leg Med. 2015;17:343-50.
133. Wang P, Yue Q. Application of IMA and H-FABP in forensic diagnosis of sudden cardiac death. Fa Yi Xue Za Zhi. 2017;33:393-6.
134. Zaborska B, Sygitowicz G, Smarż K, Pilichowska-Paszkiet E, Budaj A. Galectin-3 is related to right ventricular dysfunction in heart failure patients with reduced ejection fraction and may affect exercise capacity. Sci Rep. 2020;10:16682.
135. Zaborska B, Sikora-frąc M, Smarż K, et al. The role of galectin-3 in heart failure - the diagnostic, prognostic and therapeutic potential - where do we stand? Int J Mol Sci. 2023;24:13111.
136. Morawiec B, Kawecki D, Ho L, Tat LC, Muller O, Nowalany-Kozielska E. COPeptin for diagnosis and prediction in Acute Coronary Syndrome (COPACS) study: design and objectives. pwki. 2016;4:360-3.
137. Lin X, Lin Z, Zhao X, et al. Serum SELENBP1 and VCL are effective biomarkers for clinical and forensic diagnosis of coronary artery spasm. Int J Mol Sci. 2022;23:13266.
138. Tojo M, Shintani-Ishida K, Tsuboi H, Nakamura M, Idota N, Ikegaya H. Postmortem plasma pentraxin 3 is a useful marker of fatal acute coronary syndrome. Sci Rep. 2019;9:8090.
139. Seger C, Salzmann L. After another decade: LC-MS/MS became routine in clinical diagnostics. Clin Biochem. 2020;82:2-11.
140. Garg U, Zhang YV. Mass spectrometry in clinical laboratory: applications in biomolecular analysis. In: Garg U, Editors. Clinical applications of mass spectrometry in biomolecular analysis. New York, NY: Springer New York; 2016. pp. 1-9.
141. Martins AMA, Paiva MUB, Paiva DVN, et al. Innovative approaches to assess intermediate cardiovascular risk subjects: a review from clinical to metabolomics strategies. Front Cardiovasc. Med. 2021;8:788062.
142. Jung JY, Lee H, Kang D, et al. 1H-NMR-based metabolomics study of cerebral infarction. Stroke. 2011;42:1282-8.
143. Shirley R, Ord E, Work L. Oxidative stress and the use of antioxidants in stroke. Antioxidants. 2014;3:472-501.
144. Jaswal JS, Keung W, Wang W, Ussher JR, Lopaschuk GD. Targeting fatty acid and carbohydrate oxidation - a novel therapeutic intervention in the ischemic and failing heart. Biochim Biophys Acta Mol Cell Res. 2011;1813:1333-50.
145. Szeremeta M, Pietrowska K, Niemcunowicz-Janica A, Kretowski A, Ciborowski M. Applications of metabolomics in forensic toxicology and forensic medicine. Int J Mol Sci. 2021;22:3010.
146. Liu P, Li R, Antonov AA, et al. Discovery of metabolite biomarkers for acute ischemic stroke progression. J Proteome Res. 2017;16:773-9.
147. Kimberly WT, Wang Y, Pham L, Furie KL, Gerszten RE. Metabolite profiling identifies a branched chain amino acid signature in acute cardioembolic stroke. Stroke. 2013;44:1389-95.
148. Căținaș R, Hostiuc S. The Latest Advances in omics technology for assessing tissue damage: implications for the study of sudden cardiac death. Int J Mol Sci. 2025;26:6818.
149. Stopa V, Lileikyte G, Bakochi A, et al. Multiomic biomarkers after cardiac arrest. ICMx. 2024;12:83.
150. Galal A, Talal M, Moustafa A. Applications of machine learning in metabolomics: Disease modeling and classification. Front Genet. 2022;13:1017340.
151. Santisukwongchote K, Amornlertwatana Y, Sastraruji T, Jaikang C. Possible use of blood tryptophan metabolites as biomarkers for coronary heart disease in sudden unexpected death. Metabolites. 2019;10:6.
152. Loretz N, Becker C, Hochstrasser S, et al. Activation of the kynurenine pathway predicts mortality and neurological outcome in cardiac arrest patients: a validation study. J Crit Care. 2022;67:57-65.
153. Lv J, Pan C, Cai Y, et al. Plasma metabolomics reveals the shared and distinct metabolic disturbances associated with cardiovascular events in coronary artery disease. Nat Commun. 2024;15:5729.
154. Ma X, Sun C, Wang T, et al. A preliminary study on cause‑of‑death discrimination and the pathological stage identification in acute ischemia heart disease (AIHD) based on plasma lipidomic technique and machine learning algorithms. Int J Legal Med. 2025;139:2621-32.
155. Radaelli D, Concato M, Bruscagin T, Sinagra G, Stornaiuolo M, D’Errico S. Lipidomic profiling of hyperacute ischemic heart disease and toxic deaths: a forensic investigation into metabolic biomarkers. Int J Mol Sci. 2025;26:9031.
156. Ward LJ, Kling S, Engvall G, et al. Postmortem metabolomics as a high-throughput cause-of-death screening tool for human death investigations. iScience. 2024;27:109794.
157. Bernini Di Michele A, Onofri V, Pesaresi M, Turchi C. The role of miRNA expression profile in sudden cardiac death cases. Genes. 2023;14:1954.
158. Li LL, Zhao ZQ. The role and significance of microRNA in human cardiovascular disease and forensic science. Fa Yi Xue Za Zhi. 2013;29:39-42.(in Chinese).
159. Yan F, Chen Y, Ye X, et al. miR-3113-5p, miR-223-3p, miR-133a-3p, and miR-499a-5p are sensitive biomarkers to diagnose sudden cardiac death. Diagn Pathol. 2021;16:67.
160. Li L, He X, Liu M, Yun L, Cong B. Diagnostic value of cardiac miR-126-5p, miR-134-5p, and miR-499a-5p in coronary artery disease-induced sudden cardiac death. Front Cardiovasc Med. 2022;9:944317.
161. Singh P, Ali W, Sandhu S, et al. Post-mortem interval estimation using miRNAs of road traffic accident cases: a forensic molecular approach. Sci Justice. 2023;63:485-92.
162. Ma XN, Lu L, Huang YT, et al. Research progress of exosomal microRNA in cardiovascular disease and its forensic application prospects. Fa Yi Xue Za Zhi. 2022;38:258-62.
163. Edston E, Kawa K. Immunohistochemical detection of early myocardial infarction. An evaluation of antibodies against the terminal complement complex (C5b-9). Int J Legal Med. 1995;108:27-30.
164. Tian M, Xue J, Dai C, Jiang E, Zhu B, Pang H. CircSLC8A1 and circNFIX can be used as auxiliary diagnostic markers for sudden cardiac death caused by acute ischemic heart disease. Sci Rep. 2021;11:4695.
165. Giulian GG, Gilbert EF, Moss RL. Elevated fetal hemoglobin levels in sudden infant death syndrome. N Engl J Med. 1987;316:1122-6.
166. Vege Å, Rognum T, Scott H, Aasen A, Saugstad O. S cases have increased levels of interleukin-6 in cerebrospinal fluid. Acta Paediatr. 2008;84:193-6.
167. Buckley MG, Variend S, Walls AF. Elevated serum concentrations of β-tryptase, but not α-tryptase, in sudden infant death syndrome (SIDS). An investigation of anaphylactic mechanisms. Clin Exp Allergy. 2008;31:1696-704.
168. Duncan JR. Brainstem serotonergic deficiency in sudden infant death syndrome. JAMA. 2010;303:430.
169. Harrington CT, Hafid NA, Waters KA. Butyrylcholinesterase is a potential biomarker for sudden infant death syndrome. eBioMedicine. 2022;80:104041.
170. Haynes RL, Frelinger AL, Giles EK, et al. High serum serotonin in sudden infant death syndrome. Proc Natl Acad Sci USA. 2017;114:7695-700.
171. Opdal SH, Rognum TO, Vege Å, Saugstad OD. Hypoxanthine Levels in Vitreous Humor: a study of influencing factors in sudden infant death syndrome. Pediatr Res. 1998;44:192-6.
172. Aldridge CM, Keene KL, Normeshie CA, Mychaleckyj JC, Hauck FR. Metabolomic profiles of infants classified as sudden infant death syndrome: a case-control analysis. eBioMedicine. 2025;111:105484.
173. Osmani WA, Gallo A, Tabor M, Eilbes M, Cook-Snyder DR, Hodges MR. Repeated seizure-induced brainstem neuroinflammation contributes to post-ictal ventilatory control dysfunction. Front Physiol. 2024;15:1413479.
174. Noebels JL. Genetic and cellular mechanisms underlying SUDEP risk. In: Noebels JL, Avoli M, Rogawski MA, Vezzani A, Delgado-Escueta AV, Editors. Jasper’s basic mechanisms of the epilepsies. 5th ed. Oxford University PressNew York; 2024. pp. 1321-46.
175. Ochoa-Urrea M, Luo X, Vilella L, et al. Risk markers for sudden unexpected death in epilepsy: an observational, prospective, multicentre cohort study. The Lancet. 2025;406:1497-507.
176. Cutshaw G, Uthaman S, Hassan N, Kothadiya S, Wen X, Bardhan R. The emerging role of Raman spectroscopy as an omics approach for metabolic profiling and biomarker detection toward precision medicine. Chem Rev. 2023;123:8297-346.
177. K P S, Vadakke Matham M, Chidangil S. Recent developments in surface-enhanced Raman spectroscopy-based immuno (apta) assays for cardiac troponin detection: prospects for point-of-care applications. Biophys Rev. 2025;18:431-57.
178. Yıldırım MŞ, Akçan R. Vibrational spectroscopic techniques as a tool in diagnosis of sudden cardiac death: a systematic review. Egypt J Forensic Sci. 2025;15:37.
179. Naz M, Shafique H, Majeed MI, et al. Surface-enhanced Raman spectroscopy (SERS) for the diagnosis of acute myocardial infarction (AMI) using blood serum samples. RSC Adv. 2024;14:29151-9.
180. Huang X, Liu B, Guo S, et al. SERS spectroscopy with machine learning to analyze human plasma derived sEVs for coronary artery disease diagnosis and prognosis. Bioeng Transl Med. 2022;8:e10420.
181. Zheng P, Wu L, Raj P, et al. Multiplexed SERS detection of serum cardiac markers using plasmonic metasurfaces. Adv Sci. 2024;11:2405910.
182. Zhang T, Li B, Wuethrich A, et al. Multiplex cardiac biomarker profiling for precision coronary artery disease risk assessment using SERS with cubic core-satellite nanostructures. Anal Chem. 2025;97:14750-60.
183. Wang F, Wan H, Chen L, et al. Gemini SERS for cross-category biomarker detection and early warning of sudden cardiac death in acute coronary syndrome. ACS Nano. 2025;19:37802-14.
184. Low JSY, Teh HF, Thevarajah TM, Chang SW, Khor SM. An AI-assisted microfluidic paper-based multiplexed surface-enhanced Raman scattering (SERS) biosensor with electrophoretic removal and electrical modulation for accurate acute myocardial infarction (AMI) diagnosis and prognosis. Biosens Bioelectron. 2025;270:116949.
185. Dixon K, Bonon R, Ivander F, et al. Using machine learning and silver nanoparticle-based surface-enhanced Raman spectroscopy for classification of cardiovascular disease biomarkers. ACS Appl Nano Mater. 2023;6:15385-96.
186. Plou J, Valera PS, García I, de Albuquerque CDL, Carracedo A, Liz-Marzán LM. Prospects of surface-enhanced Raman spectroscopy for biomarker monitoring toward precision medicine. ACS photonics. 2022;9:333-50.
187. Fan Z, Li C, Cong B, Huang P. A forensic investigation of restraint stress in rats using Fourier transform infrared (FTIR) spectroscopy techniques. Microchem J. 2025;212:113212.
188. Fan Z, Li C, Sun Q, et al. Integrated analysis of restraint stress in rat serum using ATR-FTIR and Raman spectroscopy with machine learning. Spectrochim Acta A. 2025;340:126379.
189. Li X, Wan L, Ding J, et al. Investigation of biochemical alterations in the brain of db/db diabetic mice using integrated FTIR and Raman spectroscopy combined with machine learning. Spectrochim Acta A. 2026;348:127229.
190. Li X, Ding J, Fang Z, et al. FTIR spectroscopy imaging coupled with machine learning reveals biochemical changes in the brains of diabetic mice. Spectrochim Acta A. 2026;345:126835.
191. Lin H, Wang Z, Luo Y, et al. Weighted spectrochemical correlation network analysis-guided GA-PLSR: A potential spectral “fluid biopsy” approach for quantitative assessment of cardiac metabolites in diabetic cardiomyopathy. Microchem J. 2023;185:108249.
192. Dong HW, Sun Y, Qian H, et al. Research progress on postmortem changes of computed tomography imaging characteristics on corpses. Fa Yi Xue Za Zhi. 2019;35:716-20.
193. Cergan R, Taciuc IA, Dumitru M, et al. The current status of virtual autopsy using combined imaging modalities: a scoping review. JCM. 2025;14:782.
194. Tschui J, Jackowski C, Schwendener N, Schyma C, Zech WD. Post-mortem CT and MR brain imaging of putrefied corpses. Int J Legal Med. 2016;130:1061-8.
195. Jian JQ, Liu NG, Chen YJ. Research progress in virtopsy of drowning. Fa Yi Xue Za Zhi. 2019;35:328-31.
196. Grassi S, Campuzano O, Coll M, et al. Update on the diagnostic pitfalls of autopsy and post-mortem genetic testing in cardiomyopathies. Int J Mol Sci. 2021;22:4124.
197. Kimura F, Matsuo Y, Nakajima T, et al. Myocardial fat at cardiac imaging: how can we differentiate pathologic from physiologic fatty infiltration? Radiographics. 2010;30:1587-602.
198. Péporté A, Gascho D, Stamou S, et al. Evaluation of an acetated Ringer-based contrast material mixture for postmortem computed tomography angiography. Diagn Interv Imag. 2020;101:489-97.
199. Azmitia L, Grassi S, Signorelli F, et al. Post-mortem imaging of brain/spine injuries: the importance of a comprehensive forensic approach. In: Visocchi M, Editors. The funnel: from the skull base to the sacrum. Cham: Springer International Publishing; 2023. pp. 27-31.
200. Grabherr S, Egger C, Vilarino R, Campana L, Jotterand M, Dedouit F. Modern post-mortem imaging: an update on recent developments. Forensic Sci Res. 2017;2:52-64.
201. Fröhlich Knaute D, Thali MJ, Gascho D, Schweitzer W. Technical note: post mortem CT angiography of iliacofemoral arteries after cardiovascular surgery. J Forensic Radiol Imaging. 2017;9:40-3.
202. Dedouit F, Ducloyer M, Elifritz J, et al. The current state of forensic imaging - post mortem imaging. Int J Legal Med. 2025;139:1141-59.
203. Bilotta C, Perrone G, Zerbo S, et al. The multidisciplinary approach for the diagnosis of laryngohyoid lesions: a systematic literature review and meta-analysis. Clin Ter. 2023;174:97-108.
204. Jackowski C, Schwendener N, Grabherr S, Persson A. Post-mortem cardiac 3-T magnetic resonance imaging. J Am Coll Cardiol. 2013;62:617-29.
205. O’Sullivan S, Heinsen H, Grinberg LT, et al. The role of artificial intelligence and machine learning in harmonization of high-resolution post-mortem MRI (virtopsy) with respect to brain microstructure. Brain Inf. 2019;6:3.
206. Heimer J, Gascho D, Madea B, et al. Comparison of the beta-hydroxybutyrate, glucose, and lactate concentrations derived from postmortem proton magnetic resonance spectroscopy and biochemical analysis for the diagnosis of fatal metabolic disorders. Int J Legal Med. 2020;134:603-12.
207. Zoelch N, Hock A, Steuer AE, et al. In situ postmortem ethanol quantification in the cerebrospinal fluid by non-water-suppressed proton MRS. NMR Biomed. 2019;32:e4081.
208. Gascho D, Richter H, Karampinos DC, et al. Noninvasive in situ proton MRS in muscle tissue and bone marrow as a novel approach to identify previous freezing in a completely thawed cadaver. NMR Biomed. 2020;33:e4220.
209. Trayanova NA, Popescu DM, Shade JK. Machine learning in arrhythmia and electrophysiology. Circ Res. 2021;128:544-66.
210. Narayan SM, Rogers AJ. Can machine learning disrupt the prediction of sudden death? J Am Coll Cardiol. 2023;81:962-3.
211. Chen Y, Mancini M, Zhu X, Akata Z. Semi-supervised and unsupervised deep visual learning: a survey. IEEE Trans Pattern Anal Mach Intell. 2024;46:1327-47.
212. Lin M, Guo J, Gu Z, et al. Machine learning and multi-omics integration: advancing cardiovascular translational research and clinical practice. J Transl Med. 2025;23:388.
213. Osman J, Tan SC, Lee PY, Low TY, Jamal R. Sudden cardiac death (SCD) - risk stratification and prediction with molecular biomarkers. J Biomed Sci. 2019;26:39.
214. Greener JG, Kandathil SM, Moffat L, Jones DT. A guide to machine learning for biologists. Nat Rev Mol Cell Biol. 2021;23:40-55.
215. Drouard G, Mykkänen J, Heiskanen J, et al. Exploring machine learning strategies for predicting cardiovascular disease risk factors from multi-omic data. BMC Med Inform Decis Mak. 2024;24:116.
216. Pakpahan I, Sihombing M, Liu H, Wang M, Su Z, Fang M. Harnessing artificial intelligence for genomic variant prediction: advances, challenges, and future directions. GigaScience. 2026;15:giag004.
217. Fu X, Rabadan R. Understanding variants of unknown significance: the computational frontier. The Oncologist. 2024;29:653-7.
218. Hoffman-Andrews L. The known unknown: the challenges of genetic variants of uncertain significance in clinical practice. J Law Biosci. 2017;4:648-57.
219. Piraianu A, Fulga A, Musat CL, et al. Enhancing the evidence with algorithms: how artificial intelligence is transforming forensic medicine. Diagnostics. 2023;13:2992.
220. Alafer F. Emerging imaging technologies in forensic medicine: a systematic review of innovations, ethical challenges, and future directions. Diagnostics. 2025;15:1410.
221. Wichmann D, Heinemann A, Weinberg C, et al. Virtual autopsy with multiphase postmortem computed tomographic angiography versus traditional medical autopsy to investigate unexpected deaths of hospitalized patients: a cohort study. Ann Intern Med. 2014;160:534-41.
222. Li ZH, Liu NG, Dong HW, et al. Deep learning-based cardiac imaging data measurement and its application in diagnosis of sudden cardiac death. Fa Yi Xue Za Zhi. 2021;37:546-54.
223. Shen C, Lian C, Zhang W, et al. Large-vocabulary forensic pathological analyses via prototypical cross-modal contrastive learning. Nat Commun. 2025;16:6773.
224. Emani PS, Geradi MN, Gürsoy G, Grasty MR, Miranker A, Gerstein MB. Assessing and mitigating privacy risks of sparse, noisy genotypes by local alignment to haplotype databases. Genome Res. 2023;33:2156-73.
225. Zieger M, Scudder N. Ethical and legal reflections on secondary research using genetic data acquired for criminal investigation purposes. Forensic Sci Int. Genet. 2025;75:103178.
226. Amankwaa AO, Kupčuláková B, Randall K. Humanitarian forensics: stakeholder perspectives on the use of international kinship matching DNA databases. J Forensic Leg Med. 2025;116:103018.
227. Quang D, Chen Y, Xie X. DANN: a deep learning approach for annotating the pathogenicity of genetic variants. Bioinformatics. 2015;31:761-3.
228. Sundaram L, Gao H, Padigepati SR, et al. Predicting the clinical impact of human mutation with deep neural networks. Nat Genet. 2018;50:1161-70.
229. Zhou J, Troyanskaya OG. Predicting effects of noncoding variants with deep learning-based sequence model. Nat Methods. 2015;12:931-4.
230. Kelley DR, Reshef YA, Bileschi M, Belanger D, Mclean CY, Snoek J. Sequential regulatory activity prediction across chromosomes with convolutional neural networks. Genome Res. 2018;28:739-50.
231. Jaganathan K, Ersaro N, Novakovsky G, et al. Predicting expression-altering promoter mutations with deep learning. Science. 2025;389:eads7373.
232. Jaganathan K, Kyriazopoulou Panagiotopoulou S, Mcrae JF, et al. Predicting splicing from primary sequence with deep learning. Cell. 2019;176:535-548.e24.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0









Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.