


Totally endoscopic mitral valve repair employing the ten-loop technique for Barlow’s disease
 0
0 Abstract
Watch these videos of this article.

Keywords
BRIEF EXPLANATION
A 76-year-old female [height: 148 cm, weight: 46 kg, body surface area (BSA): 1.37 m2] underwent thrombectomy 4 months earlier for a cardiogenic cerebral embolism secondary to paroxysmal atrial fibrillation. Preoperative transthoracic echocardiography revealed severe mitral regurgitation due to Barlow’s disease [Video 1]. Transesophageal echocardiography (TEE) demonstrated bileaflet prolapse and annular dilatation, and surgical intervention was planned. To minimize the invasiveness in this elderly female patient and avoid median sternotomy, a totally endoscopic mitral valve repair was performed [Video 2]. To shorten the duration of cardiac arrest, five pre-formed loops of varying lengths are prepared in advance using expanded polytetrafluoroethylene (ePTFE; CV-4) [Video 3]. The main incision was a 30 mm skin incision at the right fifth intercostal space, where an extra extra small (XXS)-sized wound retractor was placed. Additional ports were inserted in the right second and third intercostal spaces, resulting in a 3-port setup. All surgical procedures were performed endoscopically without direct vision. Without leaflet resection, five artificial chordae with loops made of ePTFE (CV-4) were anchored to both the anterior and posterior papillary muscles, and ten loops were fixed to the mitral leaflets using CV-5 sutures. In addition, cryoablation for left atrial maze and left atrial appendage closure were performed to address paroxysmal atrial fibrillation. The operative time was 272 min, and the aortic cross-clamp time was 161 min. The patient was extubated on the day of surgery, drains and central venous catheter were removed on postoperative day (POD) 1, and she was discharged on POD 6 [Figure 1]. Postoperative TEE revealed no mitral regurgitation[Video 4]. Mitral valve repair for Barlow’s disease is technically demanding and associated with a high risk of recurrence[1]. The use of multiple artificial chordae enables a repair strategy that can reduce the risk of recurrent regurgitation in Barlow’s disease[2]. The loop technique enables the implantation of multiple artificial chordae[3,4]. At our institution, we routinely implant ten artificial chordae in mitral valve repair for Barlow's disease, regardless of whether leaflet resection is performed[5]. The length of the loops was determined based on measurements of the anterior and posterior leaflet lengths obtained from preoperative cardiac computed tomography (CT) and TEE, referring to the distance from the papillary muscles that would achieve an appropriate coaptation length of 5 to 10 mm. In most cases, ten artificial chordae are implanted - four longer loops attached to the anterior leaflet and six shorter loops attached to the commissural and posterior leaflets. In general, the chordae of the anterior leaflet are longer than those of the posterior leaflet, and the artificial chordae for the anterior leaflet are typically 3-5 mm longer. The ten-loops technique enabled safe and effective mitral valve repair through a totally endoscopic approach.
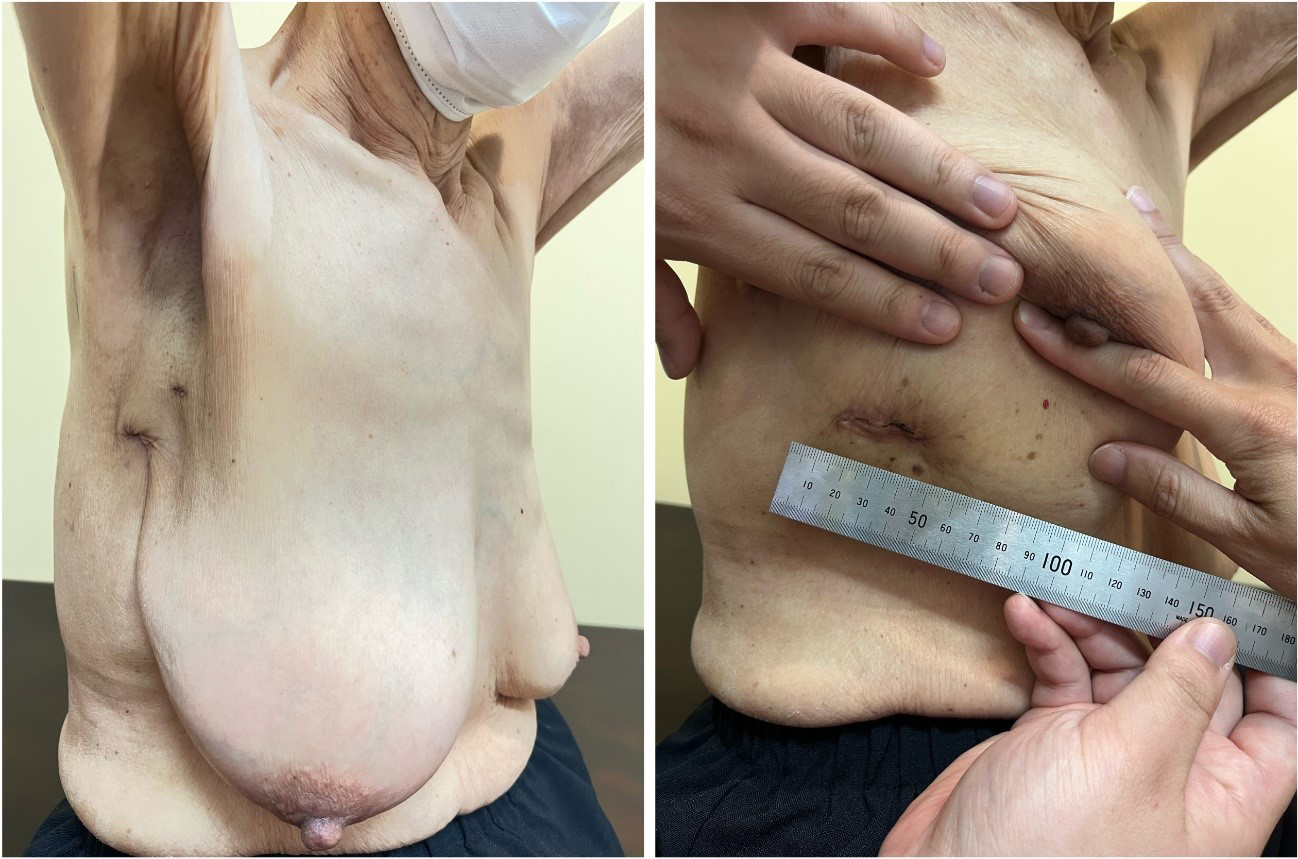
Figure 1. The figure shows the surgical wounds 30 days postoperatively. Ports were placed in the second and third intercostal spaces, and a 30-mm main incision was positioned in the sixth intercostal space along the inframammary line.
DECLARATIONS
Authors’ contributions
The author contributed solely to the article.
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
The author declares no conflicts of interest.
Ethical approval and consent to participate
This study was exempt from ethical approval because it did not involve personal information, and the Social Medical Foundation Fukuoka Wajiro Hospital Clinical Research Review Board does not require review for this type of study. All procedures were conducted in accordance with the ethical standards of the institution and the principles of the Declaration of Helsinki. Informed consent for participation and publication was obtained from the patient.
Consent for publication
Written informed consent was obtained from the patient for the publication of the accompanying images.
Copyright
© The Author(s) 2025.
Supplementary Materials
Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
REFERENCES
1. Borger MA, Kaeding AF, Seeburger J, et al. Minimally invasive mitral valve repair in Barlow’s disease: early and long-term results. J Thorac Cardiovasc Surg. 2014;148:1379-85.
2. Kasegawa H, Shimizu A, Fukui T, Takanashi S, Shimokawa T. Mitral valve repair for extreme billowing and prolapsing valve. JTCVS Open. 2022;10:169-75.
3. Shibata T, Kato Y, Motoki M, et al. Mitral valve repair with loop technique via median sternotomy in 180 patients. Eur J Cardiothorac Surg. 2015;47:491-6.
4. Takahashi Y, Abe Y, Fujii H, Morisaki A, Sakon Y, Shibata T. Loop technique for degenerative mitral regurgitation due to extended prolapse. J Card Surg. 2021;36:4485-96.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.