


Expert consensus on administering oncolytic viruses for gynecological cancers in China
 0
0 Abstract
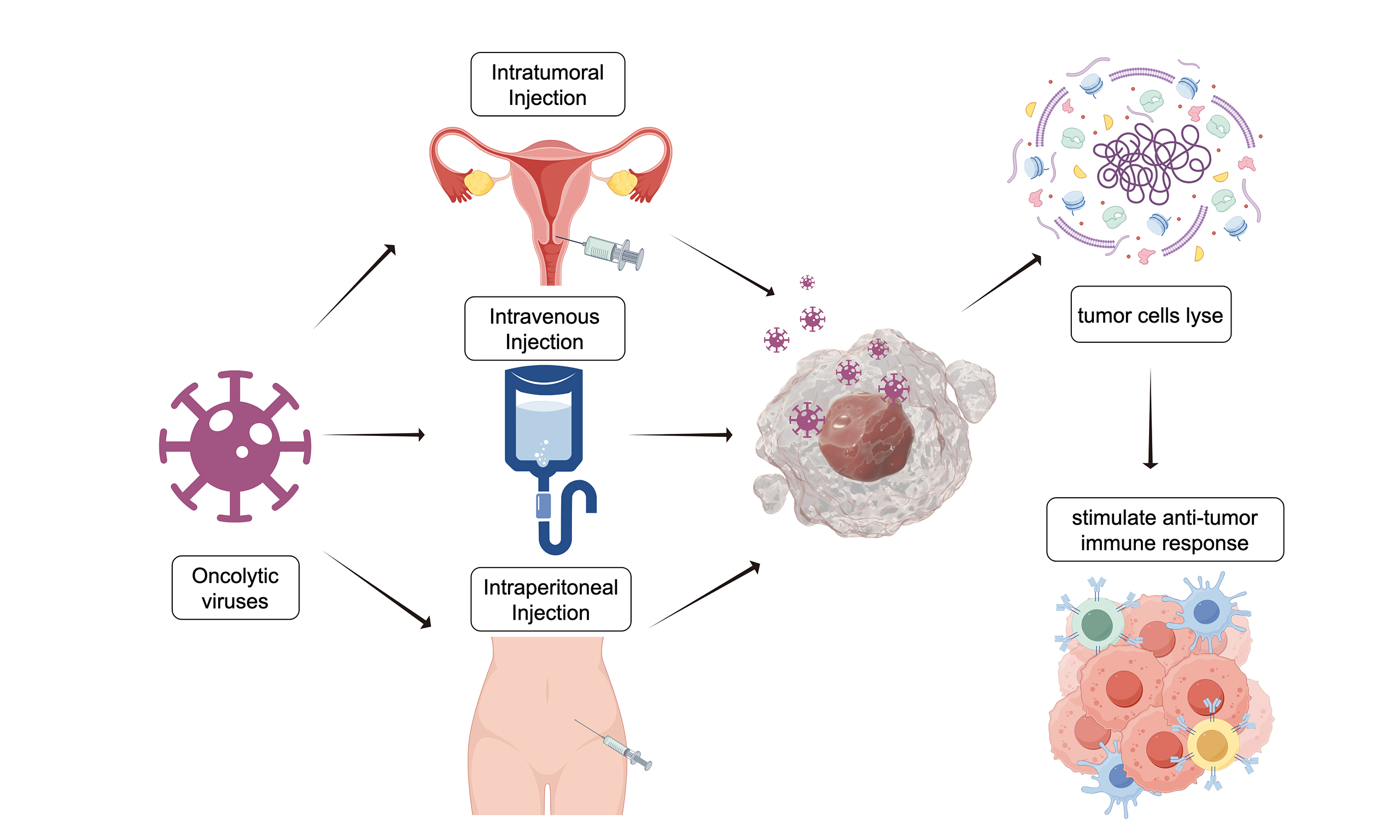
Oncolytic virus (OV) therapy constitutes a novel advancement in cancer immunotherapy, with a distinctive dual mechanism of action against gynecological malignancies. These viruses, either genetically engineered or naturally occurring, are designed to selectively replicate within and lyse tumor cells, while eliciting a robust systemic antitumor immune response through the release of tumor-associated antigens and danger signals. This therapeutic strategy shows considerable promise for treating recurrent or treatment-resistant ovarian, cervical, and endometrial cancers, conditions for which conventional therapies are often inadequate. To standardize and enhance its clinical implementation, an expert consensus evaluated and endorsed three primary routes of administration. Intratumoral injection administers the virus directly into accessible tumors, thereby maximizing local viral concentration while minimizing systemic exposure. By contrast, intravenous infusion is useful for addressing disseminated or metastatic disease, as it enables the virus to circulate and target tumor sites throughout the body. Intraperitoneal delivery is particularly significant for gynecologic malignancies, such as ovarian cancer, which predominantly metastasizes within the abdominal cavity. This approach exposes peritoneal surfaces to a high concentration of the therapeutic virus, ensuring direct interaction with both primary and metastatic lesions. By delineating these strategic administration pathways, the consensus provides a practical framework to improve efficacy, inform clinical decision-making, and facilitate the broader integration of OV therapy into the oncological treatment repertoire for gynecological cancers.
Keywords
INTRODUCTION
Oncolytic virus (OV) therapy represents a notable advancement in the biotherapeutic management of solid tumors, particularly in the context of gynecological malignancies[1-3]. These genetically engineered vectors, such as adenoviruses, herpes simplex viruses, and vaccinia viruses, are designed to selectively target and replicate within cancerous cells, while preserving normal tissue integrity. The therapeutic mechanism operates through two primary pathways: first, by inducing direct oncolysis through disruption of tumor cell membranes; and second, by enhancing systemic antitumor immunity[4,5]. This occurs through the release of tumor-associated antigens and damage-associated molecular patterns (DAMPs), which activate dendritic cells (DCs) and cytotoxic T lymphocytes. This approach shows significant promise for treating recurrent or refractory ovarian, cervical, and endometrial cancers by targeting specific tumor-related pathways, including p53 mutations and HPV-associated carcinogenesis. By modifying the immunosuppressive tumor microenvironment and enhancing tumor immunogenicity, OVs may facilitate combination approaches with other immunotherapies and exert synergistic effects when used with immune checkpoint inhibitors[6]. Current clinical applications employ various administration routes, such as intratumoral, intravenous, and intraperitoneal. Thus, ongoing research is focused on optimizing viral tropism and improving safety profiles to maximize therapeutic outcomes.
Given the established mechanisms and principles of OV therapy, and to promote its standardized and safe application in clinical settings, this consensus summarizes the key administration routes and essential operational procedures. It aligns with the expert-panel consensus in gynecologic oncology and is intended as a clinical reference.
CONSENSUS DEVELOPMENT METHODS AND PROCEDURES
Objective of consensus
By integrating advances in OV therapy technology with current treatment methodologies for gynecological malignancies and critically evaluating the evidence-based data on efficacy and safety, this approach aims to update relevant knowledge. It seeks to help healthcare professionals specializing in gynecological malignancies interpret data accurately and adjust treatment strategies accordingly. Additionally, it emphasizes the importance of providing essential education and training for patients, thereby reducing the risk of complications and improving patients' quality of life and long-term prognosis.
Users and target populations of consensus
The primary users of this consensus are gynecological oncologists and associated healthcare practitioners. Additional potential users include nurses, pharmacists, technicians, and hospital administrators. The consensus recommendations target patients diagnosed with gynecological malignancies.
Working group of consensus
The consensus panel was composed of senior experts specializing in gynecologic malignancies, with representation from gynecologic oncology, radiation oncology, medical virology, and clinical methodology. All members have substantial clinical and/or research experience in oncolytic virotherapy for gynecologic cancers, including participation in related clinical trials or guideline development. The consensus working group comprises academic advisors, a consensus writing committee, and authors. The academic advisors provided strategic oversight for the consensus development process. Their responsibilities included defining the scope of the consensus, supervising the search and evaluation of evidence, selecting experts for the consensus writing committee, and organizing consensus development meetings. The consensus writing committee was tasked with formulating the consensus outline, identifying core clinical questions, assessing the quality of evidence, and reviewing both the initial and final drafts of the consensus document. The authors were responsible for searching and organizing literature, proposing key clinical questions, performing systematic reviews on these questions, retrieving and synthesizing evidence, evaluating the quality of the evidence, drafting recommendations, preparing the initial draft, assisting in the organization of consensus discussion meetings, and integrating and revising feedback from the expert group. During the process of formulating this consensus, all members declared no direct conflicts of interest related to the content.
Identification of key consensus elements
Through a systematic review of domestic and international guidelines, expert consensus, existing systematic reviews, clinical research evidence, and expert clinical experience pertaining to the management of oncolytic viral therapy for gynecological malignancies, the authors initially compiled a list of key consensus elements. Following discussion and refinement by the expert group, this consensus delineates key elements regarding the administration of OVs for gynecological malignancies. These elements include the specific tumor types treated, a classification system for administration sites, and a detailed evaluation of various administration routes, including their respective indications, contraindications, necessary precautions, and protocols for managing adverse reactions.
Search for evidence
In accordance with the identified key methodologies, the relevant outcome indicators were evaluated, and the evidence search strategy was developed following the Population, Intervention, Comparison, and Outcome framework. The primary sources of evidence included PubMed, Web of Science, Cochrane Library, China National Knowledge Infrastructure, and Wanfang Knowledge Data Service Platform, among others. The search period covered the period from the database to September 30, 2025. The search terms included "oncolytic virus therapy", "gynecological malignancies", "cervical cancer", "ovarian cancer", and "endometrial cancer", among others. The review incorporated technical guidelines, consensus documents, systematic reviews, meta-analyses, randomized controlled trials, and observational studies. The literature screening process, outlined in Figure 1, led to the inclusion of 19 studies for further analysis. Detailed characteristics of these studies are summarized in Table 1.
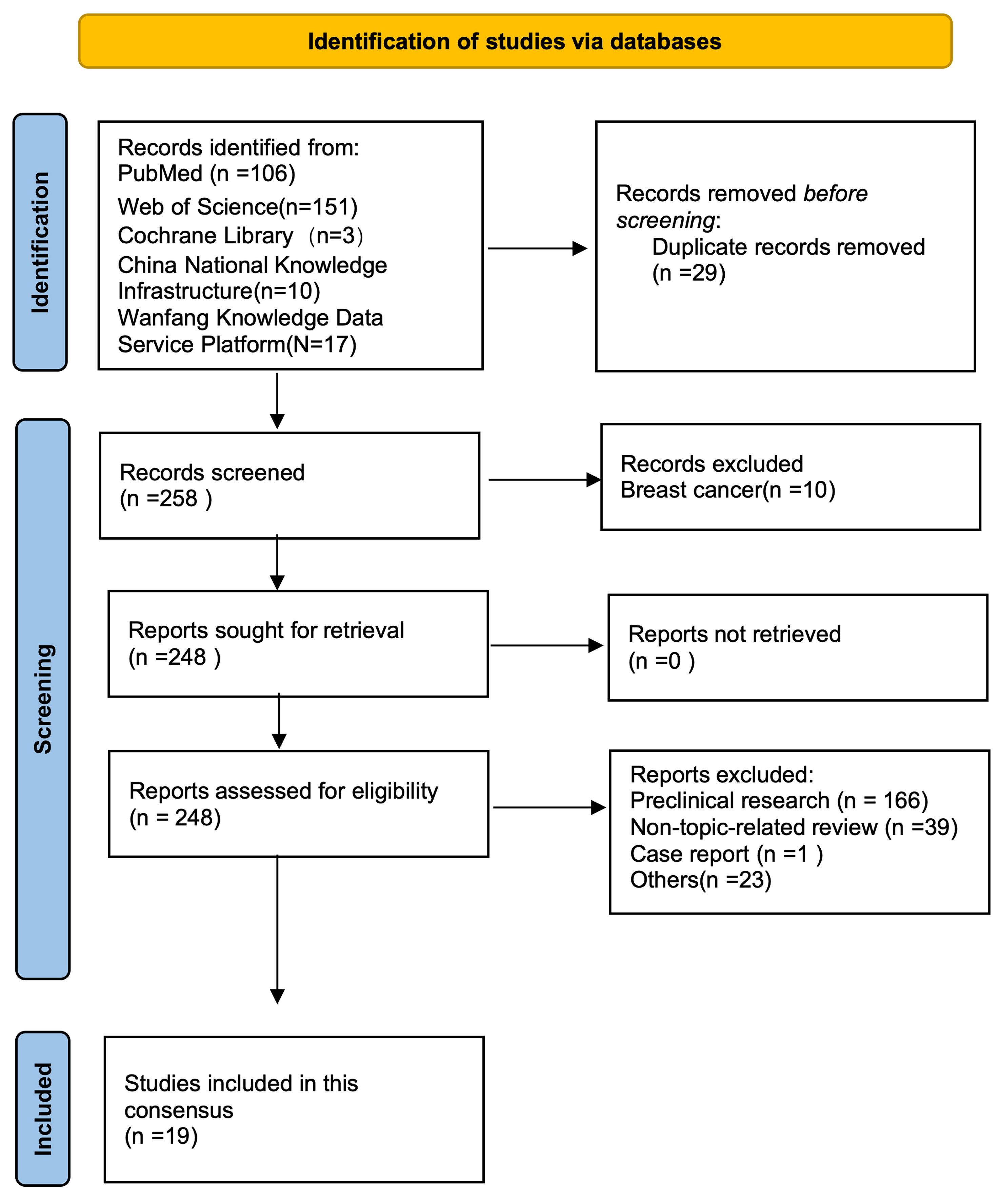
Figure 1. Literature screening flowchart.
Summary of administration routes for oncolytic virotherapy in gynecologic malignancies
| Route | Ref. | Cancer type (n) | Efficacy summary | Biologic barriers | Delivery platform | Strengths | Weaknesses | Safety |
| IT | Zhang et al., 2023[7] | Cervical (17) | ORR 70.6% (CR 9, PR 3, SD 2) | Tumor heterogeneity, necrosis, irregular distribution | H101 (Ad5) injected directly into target lesions; dose based on tumor diameter | High local concentration; low systemic exposure; direct visualization of injection | Limited to accessible lesions; not effective for metastatic disease; multiple injections needed | Grade 1-2 AEs (fever/injection site pain 35.3%); grade 3 fistula in 2 patients; no grade 4 events |
| Hemminki et al., 2015[8] | Mixed solid (ovarian n = 4) | Ovarian: mild metabolic response; tumor markers decreased in 3/4 | Tumor matrix, immune cells in TME | Ad5/3-E2F-Δ24-GMCSF; US-guided IT+low-dose IV priming | Combines IT with IV for systemic priming; personalized dosing | Requires imaging guidance; limited to injectable tumors; cyclophosphamide needed for Treg depletion | > 50% Grade 1-2 (flu/fever/fatigue/pain); Grade 3 self-limiting; no Grade 4/5 | |
| He et al., 2024[9] | Advanced solid (ovarian n = 1) | ORR 27.3%, DCR 81.8% (n = 11 evaluable) | Tumor accessibility, needle track seeding risk | YSCH-01 (oncolytic adenovirus) IT injection; dose escalation | Feasible for superficial or US-visible tumors | Single ovarian cancer case; small sample | Any AE 92.3%, grade ≥ 3 AE 7.7%; most common: fever (69.2%), nausea (30.8%), vomiting (30.8%); no DLTs, no deaths | |
| Pakola et al., 2024[10] | Advanced solid (ovarian n = 3) | DCR by PET 60%, by RECIST 20%; tumor shrinkage in injected and non-injected lesions | Heterogeneous distribution; need for multiple needle passes | TILT-123 (Ad5/3) IT+ IV; US-guided; multiple dosing days | Induces abscopal effect (response in non-injected lesions) | Complex schedule; requires a skilled interventionalist | Fever (16.7%), chills (12.8%), fatigue (8.3%). Grade 4 in 3 patients, no grade 5; no DLT | |
| Zhang et al., 2023[11] | Cervical (23) | 3-year OS 74.3%; tumor volume reduction 75.1% | Large tumor size (≥ 6 cm); fibrotic stroma | H101 injected into four quadrants of cervix; two cycles | Effective as a neoadjuvant to chemoradiotherapy; volume reduction facilitates RT | Only for locally advanced cervical cancer; requires multiple punctures | Fever (91.3%, mostly grade 1-2; grade 3 in 1 patient) and mild injection site pain (17.3%, grade 1-2) | |
| Zhang et al., 2022[12] | Gynecologic (29, mixed) | ORR 72.4%, 3-mo LC 44.8% | Lesion accessibility; injection dose titration needed | H101 IT; dose by tumor diameter (5.0 × 1011-1.5 × 1012 VP) | Practical dose adjustment; can be combined with RT/chemotherapy | Retrospective; no control group | AEs grade 1-2 (90.5%); fever 70%; one grade 4 myelosuppression; no deaths | |
| Koski et al., 2010[13] | Advanced solid (ovarian n = 4) | DCR 67% (8/12 evaluable by RECIST); antitumor activity in 62% (13/21) | Immune-mediated clearance; Tregs | Ad5/3-GMCSF IT+ 20% IV; cyclophosphamide for Treg suppression | Combines IT with low-dose IV for systemic effect | Small ovarian subgroup; old study | No grade 4-5; grade 3 in 5 patients; common grade 1-2 (fever, chills, fatigue, nausea, pain, elevated LFTs) | |
| IV | Lolkema et al., 2011[14] | Cervical (2) | DCR 80%; median SD duration 72 days | Neutralizing antibodies, complement, liver sequestration | Reovirus IV+ gemcitabine; schedule amended from days 1-5 to day 1 only | Established MTD; combination feasible | Only 2 cervical cancer cases; limited gynecologic data | Fever (69%), nausea/diarrhea/vomiting (38%-44%), chills/ALT rise (31%). Reversible grade 3 DLTs (n = 3); no deaths |
| Cohn et al., 2017 (phase IIB)[15] | Ovarian (108) | ORR 17.4% (combination) vs. 20% (paclitaxel alone); mPFS 4.4 vs. 4.3 mo | Neutralizing antibodies, rapid clearance | Reovirus IV days 1-5 + paclitaxel IV days 1,8,15 q4w | Randomized controlled trial | No PFS/OS benefit over paclitaxel alone | Grade ≥ 4 neutropenia (11.5% vs. 0%) and grade ≥ 3 respiratory events (25% vs. 2.1%) were more common with reovirus; no treatment-related deaths | |
| Pakola et al., 2024 (see IT)[10] | Ovarian (3) | DCR by PET 60% (see IT for details) | Systemic neutralization, liver uptake | TILT-123 IV on day 1 followed by IT doses | Priming dose may enhance subsequent IT effect | Small number of ovarian cancer patients | See IT row | |
| Block et al., 2025[16] | Ovarian (15) | DCR 64% (9/14), ORR 7.1% (1/14; 20% at highest dose); median PFS 98 d, median OS 190 d | Pre-existing antibodies, complement | TILT-123 IV day 1 + IT/IP days 8,22,36,57,78 + pembrolizumab | Combined with checkpoint inhibitor, acceptable safety | Phase Ia; small sample | No DLTs; most common (40% each): fever, fatigue, nausea; grade≥ 3 in 2 patients (delirium, hemoperitoneum); no treatment-related deaths | |
| Moreno et al., 2021[17] | Ovarian (38) | IV (n = 20): 4-mo PFS 64%, mPFS 6.2 mo, mOS 14.1 mo; ORR 10%, CBR 45%; CD8+ T-cell ↑ in 5/6 biopsies. IP route abandoned due to catheter complications | IP:Catheter complications (infection, pain, blockage); peritoneal complement; IV: Liver clearance (t½ 16.7 min); rapid neutralizing antibodies | IP:Enadenotucirev IP days 1,8,15 q28d; 1-6 × 1012 vp; IV:Enadenotucirev 1 × 1012 vp IV days 1,3,5 q28d + paclitaxel 80 mg/m2 days 9,16,23 | IP:Direct peritoneal delivery; IV:No catheter issues; systemic; CD8+ T-cell ↑ (5/6); virus in tumors (5 weeks); mPFS 6.2 mo, mOS 14.1 mo | IP:High catheter failure; MTD not reached; IP abandoned; IV:Grade ≥ 3 AEs 63% (neutropenia 21%); 1 possibly related death; ORR 10%; higher doses not tested (respiratory toxicity) | Grade ≥ 3 AEs in 63% (most common neutropenia 21%); 6 discontinued due to AEs; 1 possibly related death (general health deterioration); IP catheter complications frequent | |
| IP | Kim et al., 2013[18] | Ovarian (10) | Of 8 evaluable patients, 6 had stable disease, 2 progressed, and 3 had CA-125 decrease | Catheter occlusion, infection risk, and adhesions | Ad5/3-Δ24 IP daily × 3 days; Tenckhoff catheter placed ≥ 1 week prior | Well-tolerated; stable disease achieved | No objective responses; small sample | No grade 3/4 DLTs; grade 1-2 AEs (fever, nausea, fatigue, myalgia) in 5 patients. One catheter-related death (bowel perforation) |
| Kimball et al., 2010[19] | Ovarian/endometrial (21) | SD in 14/19 evaluable (74%), PD in 5; no CR/PR; CA-125 decrease in 7/20 (35%, 4 with > 20% drop) | Peritoneal adhesions, complement inactivation | Ad5/3-Δ24 IP × 3 days; dose escalation 109-1012 vp/d | Feasible dose escalation; acceptable safety | No objective responses; only SD | Grade 1-2 AEs only; no DLT/MTD reached | |
| Galanis et al., 2010[20] | Ovarian (21) | SD in 14/21 (67%), median duration 92.5 days; dose-dependent (9/9 at high doses). CA-125 drop > 30% in 5 patients; median OS 12.15 months. No CR/PR | Ascites, peritoneal membrane barriers | MV-CEA IP monthly × 6 cycles; doses 103-109 TCID50 | No DLT; dose-dependent SD/CA-125; median OS doubled (12.15 vs. 6 mo) | No PR/CR; requires laparoscopy/laparotomy for catheter placement | No DLT; only grade 1-2 toxicities (fever, fatigue, abdominal pain); one grade 3 arthralgia; no immunosuppression or shedding | |
| Zhang et al., 2024[21] | Malignant ascites (ovarian n = 3) | Median TTRP 45 days, PaFS 35 days, OS 58 days; median 1 paracentesis within 60 days. | Ascites fluid dilutes virus; complement activity | H101 1.5 × 1012 vp IP on days 1 and 3; post-injection repositioning every 5 min for 30 min | Specifically targets malignant ascites; simple procedure | Very short survival in advanced disease; small ovarian subgroup | Any grade AEs 96% (pyrexia 48%, fatigue 40%, nausea 40%); grade 3 AEs in 2 patients (8%); no grade 4 or treatment related deaths | |
| Holloway et al., 2023 (phase II)[22] | Ovarian (27) | ORR 54% (RECIST), DOR 7.6 mo, DCR 88%; CA-125 ORR 85%; mPFS 11.0 mo, mOS 15.7 mo | IP complement depletion needed; catheter-related complications | Olvi-Vec 3 × 109 pfu/d IP on 2 consecutive days via temporary catheter, followed by platinum-doublet chemotherapy ± bevacizumab | High response rate even in platinum-resistant disease; durable responses | Requires laparoscopic catheter placement; invasive | Pyrexia 63% (grade 3, 4%), abdominal pain 52% (grade 3, 7%); no grade 4/5 or treatment discontinuations | |
| Manyam et al., 2021[23] | Ovarian (12) | ORR 9%, SD 64% (SD ≥ 15w 46%), median PFS 15.7w; extended PFS in 4 pts (23.2-70.8 w); CA-125 decrease 83%; long-term survival in 3 pts (33.6-59+ mo) | PCI score, adhesions, ascites | Olvi-Vec IP monotherapy on 2 consecutive days; doses: 3 × 109, 1 × 1010, or 2.5 × 1010 PFU/day | Extended PFS in 4 patients (up to 71 weeks) | Low ORR; invasive procedure | TRAEs 100% (96% grade 1-2, 4% grade 3); no grade 4 or deaths; no DLT, MTD not reached | |
| Galanis et al., 2015[24] | Ovarian (16) | SD in 13/16 (81%), median duration 67 d; median OS 26.5 mo; 1 pathologic CR | Heavily pretreated patients; peritoneal fibrosis | MV-NIS IP every 4 weeks at 108 or 109 TCID50 | Impressive OS in platinum-resistant setting; no DLT | Non-randomized; small sample | No DLT; grade 1-2 toxicities (abdominal discomfort, fatigue, fever, neutropenia); one grade 3 event (neutropenia + bilirubin elevation) with old viral lot; no shedding | |
| Mixed/other | Kanerva et al., 2015[25] | Ovarian: 37 cases vs. 10 controls | median survival 254 vs. 74 days (P < 0.001); with CGTG-102 (n = 23) 337 vs. 74 days | Variable barriers by route | IT, IV, IP, or intrapleural per patient | Real-world, case-control design; shows survival benefit in ovarian cancer | Non-randomized; selection bias | No grade 4/5 events or treatment-related deaths; grade 3 AEs in 12 patients (mainly intestinal) |
Delphi procedure
The consensus writing group drafted each recommendation, accompanied by a summary of the supporting evidence and its assessed certainty grade. The draft and the supporting literature were subsequently reviewed and confirmed by the entire committee. To finalize the recommendations, a two-round Delphi process was used. In each round, experts rated their agreement with each item on a 5-point Likert scale: "strongly agree", "agree", "somewhat agree", "disagree", or "strongly disagree". A recommendation was considered to have achieved consensus only if at least 75% of the participating experts agreed (combining "strongly agree", "agree", and "somewhat agree").
Writing and finalization of consensus
Following the final recommendations, the expert consensus group composed the initial draft of the consensus document, which was subsequently reviewed during the consensus meeting. After incorporating the feedback, the initial draft was further revised and finalized to produce the present paper.
COMMON ROUTES OF ADMINISTRATION AND OPERATIONAL GUIDELINES
Intratumoral injection
Intratumoral injection delivers OVs directly into the tumor, eliciting a strong antitumor response. This method minimizes systemic exposure, off-target toxicity, and viral dosage while enhancing efficacy at both the injected and distant tumor sites[26]. Gynecological malignancies, such as vulvar, vaginal, cervical, and ovarian cancers, are often suitable for direct intratumoral delivery, although some deep-seated lesions require image guidance[12]. Intratumoral injection techniques are categorized into superficial and deep based on lesion depth. Superficial lesions are tumors that are either visible or palpable and can be injected directly without image guidance, such as lesions in the vulva, vagina, or cervix. Deep lesions in the uterine body, parametrium, or pelvic cavity require image-guided injection (CT or ultrasound). Oncologists can independently perform intratumoral injections for accessible lesions, whereas image-guided procedures should involve a multidisciplinary team, including oncologists and interventional radiologists[27]. The oncologist identifies suitable patients, and radiologists or sonographers assess tumor accessibility and assist with guided injections.
A clinical study by Zhang et al. evaluated the recombinant human type 5 adenovirus H101 in 17 patients with persistent or recurrent metastatic cervical cancer[7]. The overall objective response rate (ORR) was 70.6% (12/17), including 9 complete responses, 3 partial responses, and 2 cases of stable disease. Whole-exome sequencing suggested that combination therapy might enhance viral replication and immunogenic cell death through radiotherapy-induced changes in the tumor microenvironment.
Hemminki’s group developed a quadruple-genome-modified adenovirus, CGTG-602 (Ad5/3-E2F-Δ24-GMCSF), demonstrating multidimensional antitumor activity[8]. Its core design comprises: (1) a chimeric Ad5/3 fiber protein for tumor targeting; (2) an E2F-1 promoter for tumor-specific replication; (3) a Δ24 mutation disrupting Rb-mediated suppression of replication; and (4) GM-CSF gene insertion to enhance antitumor immune response. Among 12 patients with refractory solid tumors (including gynecological types), the ORR was 50%, and the disease control rate (DCR) was 83%. Adverse events (AEs) were mostly grade 1 or 2 influenza-like symptoms (fever, fatigue, and pain) and manageable; no grade 4-5 toxicities were observed. Pathological biopsies showed extensive accumulation of immune cells (particularly T cells) within tumor tissues following treatment. RNA analysis confirmed immune activation consistent with synergistic oncolytic and immunomodulatory effects.
Based on current clinical research and practice, the expert consensus on intratumoral injection is summarized as follows for reference by relevant clinical practitioners:
Indications
a. Persistent, recurrent, or metastatic gynecologic malignancies that have failed first-line therapy and lack standard treatment options.
b. Presence of at least one lesion suitable for intratumoral injection.
Lesion selection and evaluation
All tumor sites should be assessed for tumor size and needle accessibility. Superficial lesions can be injected under direct visualization regardless of size, including those < 1 cm. For deep-seated lesions, the diameter should be ≥1 cm to ensure adequate delivery and repeat dosing[26,28]. Larger lesions are generally preferred because they contain more cancer cells and release greater quantities of tumor-specific antigens, thereby enhancing T-cell activation[29]. The replication of OVs within tumors is critical for their antitumor efficacy. OVs require live cells to replicate effectively, thereby killing cancer cells and triggering antitumor immune responses[30]. However, very large lesions with central necrosis pose risks of hemorrhage and uneven drug distribution. Moreover, necrotic tumor areas, characterized by low blood flow and hypoxia, may restrict viral spread and replication[31,32]. Such an environment not only hampers viral dissemination but may also lead to viral inactivation in necrotic tissue[33]. Therefore, injections should target viable areas while avoiding necrotic regions[29,34]. To this end, image-guided assessment (e.g., ultrasound/CT) could be employed to precisely locate the viable peripheral rim and spare the necrotic core, ensuring that adjacent viable tumor cells are not missed. Tumor depth also affects needle accuracy and should be considered when selecting targets. If a treated lesion resolves but new ones appear, injections may be redirected to newly developed lesions to achieve disease control[29].
Contraindications and populations requiring caution or exclusion
a. Anticoagulation/antiplatelet therapy: Deep intratumoral injections are contraindicated in patients receiving therapeutic anticoagulants or antiplatelet agents (e.g., aspirin, clopidogrel). For prophylactic low-molecular-weight heparin, discontinue 24 h before and resume 24 h after injection. A minimum platelet count of 50 × 109/L is recommended for deep-seated tumor injections.
b. Severe hypersensitivity: Patients with a history of hypersensitivity to injectable agents (grade 3 or 4 according to the Common Terminology Criteria for Adverse Events [CTCAE]) should be excluded.
c. Vascular injury risk: Intratumoral injection is contraindicated for lesions adjacent to major blood vessels and poses a risk of vascular rupture (e.g., uterine, internal, or external iliac arteries) or those encasing major blood vessels due to vascular hemorrhage risk.
Drug dosage and schedule
An optimal dosing regimen for intratumoral OV therapy has not yet been established. Current schedules often mirror systemic chemotherapy or immune checkpoint inhibitor therapy, with injections every 2-3 weeks[26]. Multiple doses may be required to sustain local immune activation, depending on the viral vector’s replication kinetics. For example, T-VEC (herpes simplex virus-derived) persists and replicates within tumors for weeks and is administered every 2 weeks. In contrast, recombinant human type 5 adenovirus replicates rapidly but is cleared quickly, necessitating repeated injections. Clinical regimens for gynecologic tumors include daily injections for five consecutive days per cycle, repeated every 21 days[12], or injections on days 1 and 4, with a 21-day cycle[11].
Operational procedure
(1) Patient Education and Communication: Thorough pre-procedural communication is essential to ensure patients understand the surgical approach, potential complications, and expected pain levels. Pain from deep-organ puncture is typically more intense than that from superficial lesions and varies by tumor number, location, and whether biopsy is performed. Most patients do not require anesthesia; some may require local anesthesia or mild analgesia with non-steroidal anti-inflammatory drugs or weak opioids. Deep sedation or general anesthesia is rarely necessary[12,27].
(2) Procedure Preparation: A strict aseptic technique must be maintained, and all required medications must be prepared in advance.
• Superficial lesions (vulva, vagina, or cervix): Procedures should follow standard gynecological protocols, including local disinfection and manual injection[28]. Pain is usually mild and does not require preemptive analgesia.
• Deep lesions (pelvic or uterine): Local and/or systemic analgesia may be administered prior to the procedure, based on the anticipated procedural pain. Topical analgesia at the injection site can be provided with 5% lidocaine, whereas systemic analgesia may include acetaminophen, ibuprofen, or opioids, depending on the procedure specifics and the patient’s underlying symptoms[26].
For deep injections (e.g., into the uterine body or pelvis), pre-procedure coagulation testing and complete blood counts are recommended.
Although clinically approved OVs have undergone biosafety and viral shedding assessments, protective precautions remain necessary. Operators must wear gloves, masks, and goggles to prevent viral contact with skin or mucosa. Patients should avoid close contact with immunocompromised individuals or pregnant women after treatment, as viral shedding from the injection site is possible. OV preparations must be stored according to manufacturer instructions, typically at -20 to -80 °C, and prepared immediately before use to avoid repeated freeze-thaw cycles that reduce activity. Although most remain stable for several hours at room temperature, they should be administered promptly. Injection volumes should be carefully controlled: doses < 0.5 mL risk inaccurate delivery, while doses > 10 mL increase the risk of drug leakage outside the tumor[35].
(3) Image Guidance: Image-guided intratumoral injection involves three steps: needle guidance, pre-injection assessment of needle position, and post-injection evaluation[35]. The procedure, typically performed by interventional or ultrasound radiologists, can be performed under real-time ultrasound or CT guidance, with documentation of needle position through screen captures. Injection accuracy depends on tumor size, depth, and mobility. Ultrasound is generally preferred due to its real-time visualization, accessibility, low cost, and shorter procedure time. CT guidance is reserved for lesions with poor sonographic visibility or for deep-seated tumors, offering clear pre-procedural visualization of target lesions and facilitating accurate positioning. Although the injected agents themselves are not directly visible on imaging, guidance ensures accurate needle placement within the tumor.
(4) Puncture Materials: For superficial lesions (vulva or vaginal orifice), a 5-mL syringe is suitable for preparation and injection. For deep lesions (vagina, cervix, uterine body, or pelvis), needle selection depends on lesion depth. Needle gauge influences both bleeding risk and rigidity: smaller gauges lower bleeding risk but may bend more easily. Therefore, a balance between the gauge and rigidity must be considered in practical selection. Cervical carcinomas, which often exhibit abundant stromal components and firm tissue consistency, generally require an 18G (1.27 mm) needle for effective puncture and smooth delivery[12]. Deep intratumoral injections typically use a 22G (0.72 mm) needle, whereas combined biopsy and injection procedures should use an 18G (1.27 mm) coaxial needle[26]. Because OVs are not visible under CT or ultrasound, post-injection drug tracking is not feasible. To enhance safety, a Luer-Lock syringe is recommended to prevent leakage or disconnection caused by pressure changes during injection, ensuring accurate delivery[26].
(5) Injection Technique: Achieving uniform intratumoral distribution and retention of OVs remains challenging due to tumor heterogeneity. Adequate distribution of the agent across viable tumor regions is critical to maximize efficacy. Needle-based injections often result in uneven intratumoral drug distribution and fail to cover the entire tumor area. Therefore, during surgery, high-concentration drugs should be manually dispersed into as many tumor regions as possible to improve distribution. Two main percutaneous techniques are used[36].
• Fanning injection (most common): A single-entry approach where the needle is advanced to the distal end of the tumor, and the drug is injected slowly during withdrawal. Before complete withdrawal, the needle is redirected in a fan-shaped motion to distribute the drug evenly, as shown in Figure 2A. This method minimizes complications such as bleeding, pain, and leakage.
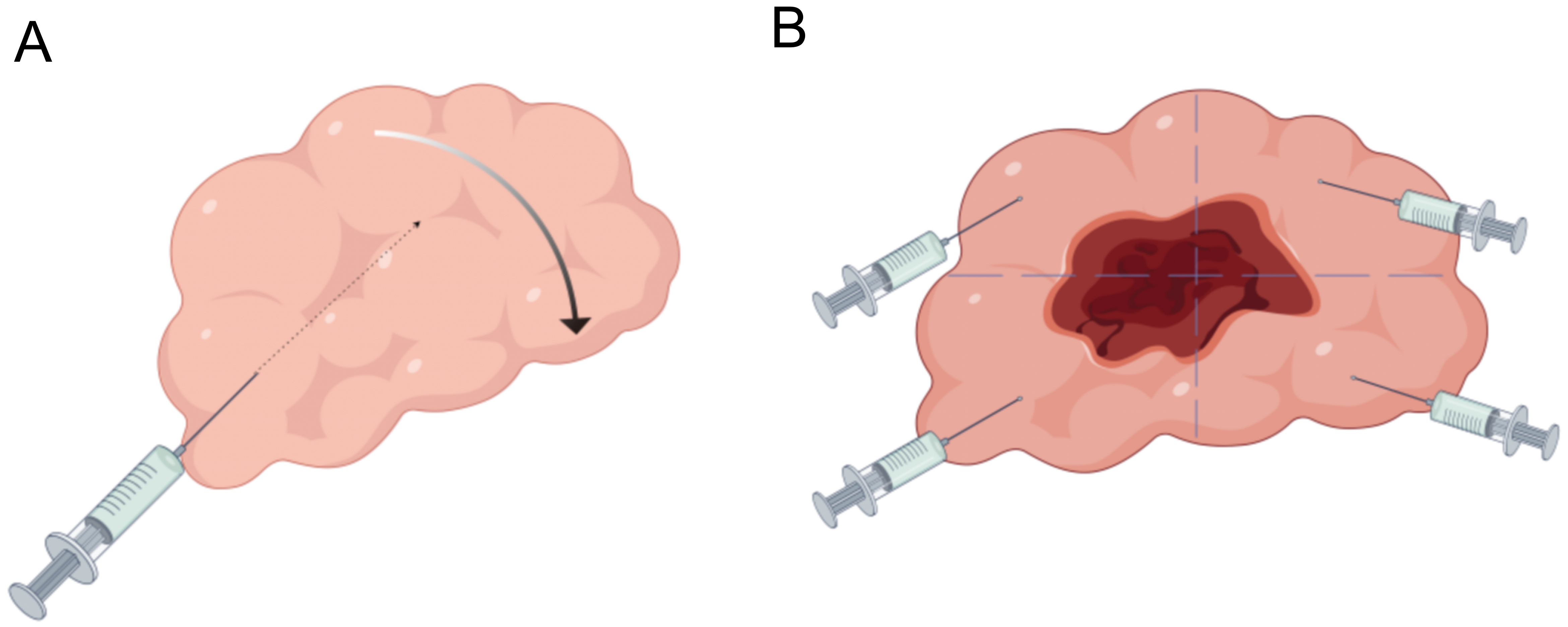
Figure 2. Schematic diagram of intratumoral injection techniques. (A) Schematic diagram of fan-shaped injection technique, Figdraw ID: TYAYTfeef9. (B) Schematic diagram of four-quadrant injection technique, Figdraw ID: YSOIRb8bcc.
• Four-quadrant technique: The needle traverses the entire lesion, delivering the agent as the needle is slowly withdrawn to cover four quadrants, ensuring uniform distribution, as shown in Figure 2B.
For patients with multiple lesions in the same organ, the same needle tract may be reused to limit drug spillage and patient/operator exposure[26]. Injection volume should account for needle dead space[26], and a small amount of air may be injected afterward to ensure full delivery of the remaining drug within the needle.
Recommendations
Intratumoral injection of OVs is appropriate for both superficial and deep lesions. A thorough evaluation of the lesion should be conducted prior to injection.
Superficial lesions measuring less than 1 cm can be injected under direct visualization, typically resulting in minimal pain and generally not requiring prior anesthesia. For deep lesions, it is advisable to select lesions
Intratumoral injections can be precisely and safely administered with the aid of imaging techniques. Real-time ultrasound and CT guidance are employed for this purpose, with ultrasound being the preferred method. CT guidance is particularly utilized for lesions or deep-seated tumors that are not well visualized with ultrasound. The guidance procedure comprises three critical steps: initial guidance, evaluation of the insertion position prior to needle insertion, and post-insertion assessment.
The "fanning injection technique" or the "four-quadrant injection technique" may be employed depending on the specific characteristics of the tumor.
Intravenous injection
While intratumoral injection is technically simple, it is limited for treating deep-seated gynecologic malignancies. Intravenous administration of OVs enables systemic delivery to multiple tumor sites, enhancing anti-metastatic activity and reducing the risk of recurrence. However, circulating antibodies and complement proteins can neutralize viral particles, limiting their accumulation in tumors when administered intravenously, and leading to their subsequent clearance by the host's humoral immune response. Strategies to prolong viral circulation and improve tumor tropism are therefore essential.
Early Phase I trials demonstrated that intravenously administered OVs, either as monotherapy or in combination with cytotoxic agents such as paclitaxel and gemcitabine, exhibited an acceptable safety profile in patients with advanced solid tumors[14,17] but showed limited efficacy. A Phase II randomized controlled trial (N = 108) by Cohn et al.[15] compared weekly paclitaxel monotherapy with paclitaxel plus the OV Reolysin® (3 × 1010 TCID50/day, days 1-5, q4w) in patients with recurrent/persistent ovarian, fallopian tube, or primary peritoneal cancer. Among 100 evaluable patients, the median progression-free survival (PFS) was 4.3 vs. 4.4 months (HR = 1.11; one-sided P = 0.687), and ORRs were 20% and 17.4%, respectively, indicating no significant clinical benefit. The combination group showed higher rates of severe neutropenia and respiratory events (12% vs. 0% and 25% vs. 2%, respectively), as well as more frequent fever, myalgia, and headache. No treatment-related deaths occurred.
Systemic delivery faces major biological barriers that reduce OVs’ bioavailability. To overcome these barriers, several innovative nanotechnology-based delivery systems have been developed. He et al. developed a nanocapsule encapsulating the recombinant OV EV-A71-miR124T, enabling the virus to cross the blood-brain barrier and selectively release at tumor sites. This approach suppressed intracranial tumor growth and significantly prolonged survival in mouse glioma models[37]. Xu et al. developed AD@PSSP, a multifunctional adenovirus-based nanodelivery system functionalized with a polyethyleneimine-polyethylene glycol (PEI-PEG) coating, thereby improving systemic stability and tumor targeting[38]. Zhong et al. constructed a recombinant Newcastle disease virus carrying the porcine α1,3GT gene (NDV-GT) via reverse genetics. In preclinical primate models and a clinical trial (N = 20) for relapsed/refractory metastatic cancer, NDV-GT achieved a 90.00% DCR and durable responses, with no serious AEs or neutralizing antibodies detected[39]. Collectively, these advances highlight the potential of intravenous OV therapy, especially when combined with nanotechnology, to improve systemic delivery, safety, and efficacy against deep or metastatic tumors.
Recommendations
Intravenous OVs can be delivered systemically to multiple tumor sites, thereby enhancing anti-metastatic activity and reducing the risk of recurrence. This approach is particularly suitable for treating tumors located deep within the body as well as multiple tumors. Developing strategies to extend the circulation time of these viruses and to enhance their tumor tropism are essential.
Intraperitoneal injection
Intraperitoneal administration of OVs offers localized delivery within the peritoneal cavity, thereby overcoming some limitations of systemic therapy. This route enables high local viral concentrations, targeted immune modulation, and improved drug penetration. A preclinical study demonstrated that intraperitoneal injection of recombinant vaccinia virus GLV-0b347 in a mouse model prolonged survival and reduced ascites formation[40]. Multiple Phase I studies confirmed its feasibility and safety in patients with recurrent, advanced, and refractory gynecologic malignancies, particularly ovarian cancer[18-20]. In a Phase II trial (NCT04771676), Zhang et al. evaluated intraperitoneal H101 in 25 patients with malignant ascites[21]. The median time to repeat paracentesis was 45 days, compared with 13 days in the control group. Treatment-related AEs occurred in 96% of patients, most commonly fever (48%), fatigue (40%), nausea (40%), abdominal pain (32%), and chills (20%). Two patients (8%) experienced grade 3 AEs (abdominal pain and anemia), with no grade 4 events or deaths. Single-cell analysis revealed robust oncolysis, early viral replication, and enhanced CD8+ T-cell-macrophage immune checkpoint interactions[21]. Further evidence came from a Phase II single-arm study conducted by Holloway et al. (N = 27), evaluating intraperitoneal Olvi-Vec in patients with platinum-resistant or platinum-refractory ovarian cancer[22]. A temporary intraperitoneal catheter was placed via laparoscopy, followed by Olvi-Vec (3 × 109 plaque-forming units [pfu] daily for 2 days) and subsequent platinum-based chemotherapy ± bevacizumab. After a median follow-up of 47.0 months, key outcomes included: ORR 54% (RECIST 1.1), median DOR 7.6 months, DCR 88%, median PFS 11.0 months, and median OS 15.7 months overall (18.5 months in platinum-resistant; 14.7 months in platinum-refractory subgroups). Common treatment-related AEs included fever (63.0%; grade 3.7%) and abdominal pain (51.9%; grade 7.4%). No grade 4 AEs, treatment discontinuations, or deaths occurred. These findings suggest that Olvi-Vec plus platinum-based chemotherapy provides meaningful clinical benefit with acceptable safety[22]. Based on these findings, the FDA granted Fast Track designation to Olvi-Vec in November 2023. Based on the aforementioned evidence, the Phase III OnPrime study (GOG-3076, NCT05281471) is now underway[41]. This multicenter, randomized, active-controlled trial aims to enroll
Recommendations
Intraperitoneal administration of OVs delivers them locally into the abdominal cavity, thereby addressing some limitations of systemic therapy. This approach enables higher local concentrations of the virus, targeted immunomodulation, and enhanced drug penetration, which is particularly advantageous for treating platinum-resistant or platinum-refractory ovarian cancer.
Management of adverse reactions
OV administration is generally well-tolerated. The most common adverse reactions include influenza-like symptoms, local injection-site reactions, fever, nausea, vomiting, and decreased appetite[9,42]. These symptoms usually resolve spontaneously, often after a brief treatment interruption or dose withholding. In cases of poor tolerance or significant fever, symptomatic management can usually restore normal body temperature. Local reactions, such as pain, rash, erythema, and peripheral edema, are generally self-limiting. When OVs are combined with other antitumor therapies, including radiotherapy or chemotherapy, adverse reactions may occur, such as hematologic toxicities (anemia, leukopenia, neutropenia, thrombocytopenia) or hepatic dysfunction. These toxicities can be managed with standard supportive measures. AEs associated with recombinant OVs should be evaluated and graded according to the CTCAE, version 6.0, issued by the National Cancer Institute.
Grade 1 or 2 events: Symptomatic management is recommended, and treatment may continue under close monitoring.
Grade 3 or higher events: Urgent intervention is advised, and oncolytic virotherapy should be discontinued.
Handling OVs must comply with Biosafety Level 2 (BSL-2) standards and institutional protocols, including disinfection of equipment and work surfaces with appropriate agents, such as a ≥ 2% bleach solution[15].
Recommendations
1. OV administration is usually well-tolerated, with common side effects like flu-like symptoms, injection-site reactions, fever, nausea, vomiting, and reduced appetite. These symptoms typically resolve on their own, often after a short treatment pause or dose adjustment.
2. When OVs are used alongside other cancer treatments, AEs linked to recombinant oncolytic adenoviruses should be assessed using CTCAE version 6.0. For grade 1 or 2 events, manage symptoms and continue treatment with careful monitoring. For grade 3 or higher events, urgent intervention is needed, and virotherapy should be stopped.
DISCUSSION
OVs represent a novel therapeutic approach in oncology, with substantial potential for clinical application in gynecological malignancies. Recent advancements in OV therapy research have been notable across various cancer types, with a pronounced focus on gynecological malignancies, where OV therapy has demonstrated promising therapeutic outcomes. Currently, in addition to published experimental findings, numerous clinical trials are actively investigating the application of OVs in the treatment of gynecological malignancies. Further details are provided in Table 2.
Active oncolytic virus clinical trials by route of administration
| Route of administration | NCT number | Study title | Oncolytic virus | Enrollment | Phase | Key indications | Country |
| Intratumoral | NCT06265025 | GM103 Intratumoral Injection in Locally Advanced/Metastatic Solid Tumors | GM103 | 125 | Phase 1/2 | Head and Neck Cancer, Malignant Melanoma, Colorectal Cancer, Renal Cell Carcinoma, Cervical Cancer, Breast Cancer | South Korea |
| NCT06311578 | JNJ-87704916 as Monotherapy and in Combination for Advanced Solid Tumors | JNJ-87704916 | 96 | Phase 1 | Neoplasms | USA | |
| NCT07128914 | GO306 in Patients with Advanced Solid Tumors | GO306 | 32 | Phase 1 | Solid Tumor Malignancies | China | |
| NCT06368921 | Recombinant Oncolytic Virus M1 (VRT106) in patients with Solid Tumors | VRT106 | 30 | Phase 1 | Solid Tumor | China | |
| NCT06883149 | PIN in Combination with Anti-PD1 in Previously Treated Solid Tumor | PIN | 25 | Phase 1 | Solid Tumor | China | |
| ChiCTR2500103773 | Combination therapy of oncolytic vaccinia virus and PD-1 inhibitor in advanced solid tumors | hV01 | 24 | Phase 1 | Advanced solid tumors | China | |
| NCT06508307 | Intratumoral Injection Oncolytic Vaccinia Virus GC001 in Advanced Solid Tumors | GC001 | 21 | Phase 1 | Sarcoma, Cervical Cancer, Colon Cancer, Lung Cancer, Ovarian Cancer, Pancreatic Cancer, Hepatocellular Carcinoma, Breast Cancer, Gastric Cancer | China | |
| Intravenous | NCT06910657 | IDOV-Immune for Advanced Solid Tumors | IDOV-Immune (oncolytic vaccinia virus) | 78 | Phase 1 | Colorectal Cancer, Pancreatic Cancer, Melanoma, Ovarian Cancer, Gastric Cancer, Esophageal Cancer, Hepatocellular Carcinoma, Renal Cell Carcinoma, Breast Cancer, Sarcoma, Bladder Cancer, Lung Cancer, Prostate Cancer, Cervical Cancers, Head and Neck Cancers, Adrenal Gland Tumors | USA |
| NCT07231458 | ABX-001 Alone and in Combination with Pembrolizumab for Refractory/Relapsed Advanced Solid Tumors | ABX-001 | 27 | Phase 1 | Advanced Solid Tumors | Germany | |
| NCT06826313 | Intravenous VRT106 for Locally Advanced or Metastatic Solid Tumors | VRT106 | 12 | Phase 1 | Solid Tumors | China | |
| NCT06046742 | Intravenous M1-c6v1 for Locally Advanced or Metastatic Solid Tumors | M1-c6v1 | 12 | Phase 1 | Solid Tumor | China | |
| Intraperitoneal | NCT05684731 | KM1 in Subjects with recurrent or Refractory Ovarian Cancer | KM1 | 30 | Phase 1 | Ovarian Cancer | China |
| NCT07211659 | THEO-260 via Intraperitoneal Route in Ovarian Cancer (OCTOPOD-IP) | THEO-260 | 18 | Phase 1 | Ovarian Cancer | United Kingdom | |
| Intratumoral and/or intraperitoneal | NCT05271318 | TILT-123 + Pembrolizumab ± Pegylated Liposomal Doxorubicin in Ovarian Cancer (PROTA) | TILT-123 | 29 | Phase 1/1b | Platinum-resistant/refractory ovarian, fallopian tube, and primary peritoneal carcinomas | Finland |
| Intratumoral or intraperitoneal | NCT05281471 | Olvi-Vec + Platinum-doublet + Bevacizumab in Platinum-Resistant/Refractory Ovarian Cancer (OnPrime) | Olvi-Vec | 186 | Phase 3 | Platinum-resistant/refractory ovarian, fallopian tube, and primary peritoneal cancers | USA |
The antitumor efficacy of OVs is largely mediated by the host immune system. OV infection induces immunogenic cell death, releasing DAMPs and pathogen-associated molecular patterns (PAMPs). These molecules activate innate immune cells via pattern recognition receptors, trigger type I interferon responses, and recruit DCs and natural killer cells. DCs subsequently cross-present tumor antigens to CD8+ T cells, thereby initiating systemic adaptive immune responses[43]. The tumor microenvironment in gynecologic cancers is often immunosuppressive, characterized by abundant regulatory T cells, myeloid-derived suppressor cells, and M2 macrophages[44]. OVs can partially reverse this suppression by lysing immunosuppressive cells and producing chemokines that attract effector T cells; however, OV infection also upregulates PD-L1 expression as an adaptive resistance mechanism[45]. The STING pathway, activated by cytosolic DNA generated during OV replication, is essential for type I interferon production and CD8+ T cell cross-priming; defective STING signaling impairs oncolytic efficacy[46]. OVs can also induce inflammasome activation, pyroptosis, and metabolic reprogramming that affect T cell function[47].
Clinical data support the therapeutic potential of OVs in gynecologic tumors[3]. OVs can also be combined with radiotherapy, chemotherapy, and particularly immunotherapy, and such combinations hold considerable promise for enhancing treatment efficacy[34,48]. As a novel cancer therapeutic modality, OVs selectively replicate within tumor cells and induce immunogenic cell death, thereby activating antitumor immune responses[36,49]. In the context of immunotherapy, OVs facilitate immune activation by releasing tumor-associated antigens and danger signals, which in turn augment antitumor immunity[50]. For instance, the combination of OVs with immune checkpoint inhibitors has demonstrated favorable results in multiple clinical trials, converting “cold" tumor microenvironments into “hot" ones and enhancing immune cell infiltration[6,51]. Therefore, the treatment sequence is particularly important. Studies using murine models have indicated that administering OVs prior to the activation of natural killer T cells yields significantly greater efficacy than the reverse sequence. This enhanced effectiveness is likely due to OV-induced immunogenic cell death and the subsequent activation of the immune system[52]. Furthermore, additional studies have demonstrated that the combination of OVs with T-cell transfer therapy not only improves therapeutic outcomes but also remodels the tumor microenvironment and enhances T-cell recruitment[53]. In addition, OVs can be combined with CAR-T cell therapy to promote CAR-T cell infiltration into tumors and restore their functional activity, thereby increasing therapeutic efficacy[54]. Synergistic effects have also been observed when OVs are combined with radiotherapy and chemotherapy. Mechanistically, OVs enhance radiotherapy-induced DNA damage and improve the intratumoral distribution of chemotherapeutic agents[38,55]. In addition, OVs remodel the tumor microenvironment, thereby potentiating the efficacy of both chemotherapy and radiotherapy[56]. However, several challenges remain, including inefficient systemic viral delivery, rapid immune clearance, and the immunosuppressive tumor microenvironment. Systemic delivery of OVs remains particularly difficult. To address these obstacles, researchers are developing novel delivery systems, such as cellular carriers, to improve OV distribution within tumors and immune activation [57,58]. Nanotechnology is also being employed to enhance the stealth properties and tumor specificity of OVs, thereby increasing their overall therapeutic efficacy[59].
To date, the evidence on oncolytic virotherapy for gynecologic malignancies is primarily derived from small-sample, single-arm studies, with a paucity of high-quality randomized controlled trials. This limitation reflects the early stage of clinical development rather than a lack of therapeutic promise. Accumulating data support favorable antitumor activity and safety. Given the nature of the available evidence, this consensus does not provide definitive comparative conclusions across routes of administration. Instead, it focuses on a systematic characterization of each route, including indications, contraindications, precautions, and AE management, thereby offering practical clinical guidance for physicians.
CONCLUSION
OV therapy has demonstrated potential in the treatment of gynecologic cancers, particularly in cases of recurrence and metastasis. Progress in delivery systems and the integration of this therapy with existing treatments may enhance therapeutic efficacy and expand clinical applications, thereby improving patient outcomes.
DECLARATIONS
Acknowledgement
The graphical abstract was created using FigDraw, and the copyright ID is RSYYO27ac4.
Authors’ contributions
Conducted the literature search; formulated key clinical questions; performed the systematic review; retrieved and synthesized evidence; assessed evidence quality; drafted recommendations; prepared the initial draft; assisted in organizing consensus discussion meetings; and integrated and revised feedback: Zang L,
Provided strategic oversight of consensus development (as academic advisor); defined the scope of the consensus; supervised evidence search and evaluation; selected members of the consensus writing committee; organized consensus development meetings; and critically reviewed the consensus document: Zhang Q
Provided strategic oversight (as academic advisor); assessed evidence quality; participated in consensus development meetings; provided methodological guidance; and approved the final consensus draft: Zhang K
Supervised the overall consensus process; provided final approval of the consensus document; coordinated the consensus panel; and fulfilled the responsibilities of the corresponding author: Xu Q
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this work, the AI tool DeepSeek (version R1, released 2025-01-20) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This work was funded by the Fujian Province Joint Innovation Funds (2024Y9593), the Fujian Province Natural Science Foundation (2023J011250) and the Clinical Research Grant of Fujian Cancer Hospital (202413008).
Conflicts of interest
Xu Q is the Guest Editor of the Special Issue “Multimodal and Personalized Approaches for Cervical Cancer Treatment" of Journal of Cancer Metastasis and Treatment. Xu Q was not involved in any steps of the editorial processing, notably including reviewer selection, manuscript handling, or decision making, while the other authors have declared that they have no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Alwithenani A, Hengswat P, Chiocca EA. Oncolytic viruses as cancer therapeutics: from mechanistic insights to clinical translation. Mol Ther. 2025;33:2217-28.
2. Hartkopf AD, Fehm T, Wallwiener D, Lauer U. Oncolytic virotherapy of gynecologic malignancies. Gynecol Oncol. 2011;120:302-10.
3. Kumar N. Infecting cancer to cure it: the power of oncolytic viruses in gynecologic oncology - a narrative review. Drug Res. 2025;75:261-74.
4. Chiocca EA, Rabkin SD. Oncolytic viruses and their application to cancer immunotherapy. Cancer Immunol Res. 2014;2:295-300.
5. Donnelly O, Harrington K, Melcher A, Pandha H. Live viruses to treat cancer. J R Soc Med. 2013;106:310-4.
6. Larocca CJ, Warner SG. Oncolytic viruses and checkpoint inhibitors: combination therapy in clinical trials. Clin Transl Med. 2018;7:e35.
7. Zhang Q, Zhang J, Liu Z, et al. Recombinant human adenovirus type 5 (H101) intra-tumor therapy in patients with persistent, recurrent, or metastatic cervical cancer: genomic profiling relating to clinical efficacy. Drug Des Devel Ther. 2023;17:3507-22.
8. Hemminki O, Parviainen S, Juhila J, et al. Immunological data from cancer patients treated with Ad5/3-E2F-Δ24-GMCSF suggests utility for tumor immunotherapy. Oncotarget. 2015;6:4467-81.
9. He Y, Huang X, Li X, et al. Preliminary efficacy and safety of YSCH-01 in patients with advanced solid tumors: an investigator-initiated trial. J Immunother Cancer. 2024;12:e008999.
10. Pakola SA, Peltola KJ, Clubb JH, et al. Safety, efficacy, and biological data of T-Cell-enabling oncolytic adenovirus TILT-123 in advanced solid cancers from the TUNIMO monotherapy phase I trial. Clin Cancer Res. 2024;30:3715-25.
11. Zhang X, Wang Y, Lv X, et al. Intratumoral injection of oncolytic virus (H101) in combination with concurrent chemoradiotherapy for locally advanced cervical cancer. Int J Gynecol Cancer. 2023;33:1051-6.
12. Zhang J, Zhang Q, Liu Z, et al. Efficacy and safety of recombinant human adenovirus type 5 (H101) in persistent, recurrent, or metastatic gynecologic malignancies: a retrospective study. Front Oncol. 2022;12:877155.
13. Koski A, Kangasniemi L, Escutenaire S, et al. Treatment of cancer patients with a serotype 5/3 chimeric oncolytic adenovirus expressing GMCSF. Mol Ther. 2010;18:1874-84.
14. Lolkema MP, Arkenau H, Harrington K, et al. A phase I study of the combination of intravenous reovirus type 3 dearing and gemcitabine in patients with advanced cancer. Clin Cancer Res. 2011;17:581-8.
15. Cohn DE, Sill MW, Walker JL, et al. Randomized phase IIB evaluation of weekly paclitaxel versus weekly paclitaxel with oncolytic reovirus (Reolysin®) in recurrent ovarian, tubal, or peritoneal cancer: an NRG Oncology/Gynecologic Oncology Group study. Gynecol Oncol. 2017;146:477-83.
16. Block MS, Clubb JHA, Mäenpää J, et al. The oncolytic adenovirus TILT-123 with pembrolizumab in platinum resistant or refractory ovarian cancer: the phase 1a PROTA trial. Nat Commun. 2025;16:1381.
17. Moreno V, Barretina-Ginesta M, García-Donas J, et al. Safety and efficacy of the tumor-selective adenovirus enadenotucirev with or without paclitaxel in platinum-resistant ovarian cancer: a phase 1 clinical trial. J Immunother Cancer. 2021;9:e003645.
18. Kim KH, Dmitriev IP, Saddekni S, et al. A phase I clinical trial of Ad5/3-Δ24, a novel serotype-chimeric, infectivity-enhanced, conditionally-replicative adenovirus (CRAd), in patients with recurrent ovarian cancer. Gynecol Oncol. 2013;130:518-24.
19. Kimball KJ, Preuss MA, Barnes MN, et al. A phase I study of a tropism-modified conditionally replicative adenovirus for recurrent malignant gynecologic diseases. Clin Cancer Res. 2010;16:5277-87.
20. Galanis E, Hartmann LC, Cliby WA, et al. Phase I trial of intraperitoneal administration of an oncolytic measles virus strain engineered to express carcinoembryonic antigen for recurrent ovarian cancer. Cancer Res. 2010;70:875-82.
21. Zhang Y, Qian L, Chen K, et al. Oncolytic adenovirus in treating malignant ascites: A phase II trial and longitudinal single-cell study. Mol Ther. 2024;32:2000-20.
22. Holloway RW, Mendivil AA, Kendrick JE, et al. Clinical activity of olvimulogene nanivacirepvec-primed immunochemotherapy in heavily pretreated patients with platinum-resistant or platinum-refractory ovarian cancer: the nonrandomized phase 2 VIRO-15 clinical trial. JAMA Oncol. 2023;9:903.
23. Manyam M, Stephens AJ, Kennard JA, et al. A phase 1b study of intraperitoneal oncolytic viral immunotherapy in platinum-resistant or refractory ovarian cancer. Gynecol Oncol. 2021;163:481-9.
24. Galanis E, Atherton PJ, Maurer MJ, et al. Oncolytic measles virus expressing the sodium iodide symporter to treat drug-resistant ovarian cancer. Cancer Res. 2015;75:22-30.
25. Kanerva A, Koski A, Liikanen I, et al. Case-control estimation of the impact of oncolytic adenovirus on the survival of patients with refractory solid tumors. Mol Ther. 2015;23:321-9.
26. Marabelle A, Andtbacka R, Harrington K, et al. Starting the fight in the tumor: expert recommendations for the development of human intratumoral immunotherapy (HIT-IT). Ann Oncol. 2018;29:2163-74.
27. Sheth RA, Murthy R, Hong DS, et al. Assessment of image-guided intratumoral delivery of immunotherapeutics in patients with cancer. JAMA Netw Open. 2020;3:e207911.
28. Tselikas L, Champiat S, Sheth RA, et al. Interventional radiology for local immunotherapy in oncology. Clin Cancer Res. 2021;27:2698-705.
29. Goldmacher GV, Khilnani AD, Andtbacka RHI, et al. Response criteria for intratumoral immunotherapy in solid tumors: itRECIST. J Clin Oncol. 2020;38:2667-76.
30. Twumasi-Boateng K, Pettigrew JL, Kwok YYE, Bell JC, Nelson BH. Oncolytic viruses as engineering platforms for combination immunotherapy. Nat Rev Cancer. 2018;18:419-32.
31. Miller A, Nace R, Ayala-Breton CC, et al. Perfusion pressure is a critical determinant of the intratumoral extravasation of oncolytic viruses. Mol Ther. 2016;24:306-17.
32. Breitbach CJ, De Silva NS, Falls TJ, et al. Targeting tumor vasculature with an oncolytic virus. Mol Ther. 2011;19:886-94.
33. Bayona C, Ranđelović T, Ochoa I. Tumor microenvironment in glioblastoma: the central role of the hypoxic-necrotic core. Cancer Lett. 2026;639:218216.
34. Tacher V, Le Deley MC, Hollebecque A, et al. Factors associated with success of image-guided tumour biopsies: Results from a prospective molecular triage study (MOSCATO-01). Eur J Cancer. 2016;59:79-89.
35. Sheth RA, Wehrenberg-Klee E, Patel SP, Brock KK, Fotiadis N, De Baère T. Intratumoral injection of immunotherapeutics: state of the art and future directions. Radiology. 2024;312:e232654.
36. Shalhout SZ, Miller DM, Emerick KS, et al. Therapy with oncolytic viruses: progress and challenges. Nat Rev Clin Oncol. 2023;20:160-77.
37. He Y, Li W, Zhang X, Cui Z. Oncolytic virus targeted therapy for glioma via intravenous delivery. Adv Healthc Mater. 2025;14:2404965.
38. Xu C, Chen L, Liu G, et al. Tailoring an intravenously injectable oncolytic virus for augmenting radiotherapy. Cell Rep Med. 2025;6:102078.
39. Zhong L, Gan L, Wang B, et al. Hyperacute rejection-engineered oncolytic virus for interventional clinical trial in refractory cancer patients. Cell. 2025;188:1119-36.e23.
40. Jazowiecka-Rakus J, Hadrys A, Rahman MM, et al. Myxoma virus expressing LIGHT (TNFSF14) pre-loaded into adipose-derived mesenchymal stem cells is effective treatment for murine pancreatic adenocarcinoma. Cancers. 2021;13:1394.
41. Holloway RW, Thaker P, Mendivil AA, et al. A phase III, multicenter, randomized study of olvimulogene nanivacirepvec followed by platinum-doublet chemotherapy and bevacizumab compared with platinum-doublet chemotherapy and bevacizumab in women with platinum-resistant/refractory ovarian cancer. Int J Gynecol Cancer. 2023;33:1458-63.
42. Macedo N, Miller DM, Haq R, Kaufman HL. Clinical landscape of oncolytic virus research in 2020. J Immunother Cancer. 2020;8:e001486.
43. Gujar S, Pol JG, Kim Y, Lee PW, Kroemer G. Antitumor benefits of antiviral immunity: an underappreciated aspect of oncolytic virotherapies. Trends Immunol. 2018;39:209-21.
44. Santoiemma PP, Powell DJ. Tumor infiltrating lymphocytes in ovarian cancer. Cancer Biol Ther. 2015;16:807-20.
45. Russell SJ, Barber GN. Oncolytic viruses as antigen-agnostic cancer vaccines. Cancer Cell. 2018;33:599-605.
46. Woo S, Fuertes MB, Corrales L, et al. STING-dependent cytosolic DNA sensing mediates innate immune recognition of immunogenic tumors. Immunity. 2014;41:830-42.
47. Guo ZS, Liu Z, Bartlett DL. Oncolytic immunotherapy: dying the right way is a key to eliciting potent antitumor immunity. Front Oncol. 2014;4:74.
48. Zhang B, Cheng P. Improving antitumor efficacy via combinatorial regimens of oncolytic virotherapy. Mol Cancer. 2020;19:158.
49. Hemminki O, Dos Santos JM, Hemminki A. Oncolytic viruses for cancer immunotherapy. J Hematol Oncol. 2020;13:84.
50. de Graaf J, De Vor L, Fouchier R, Van Den Hoogen B. Armed oncolytic viruses: a kick-start for anti-tumor immunity. Cytokine Growth Factor Rev. 2018;41:28-39.
51. Crunkhorn S. Oncolytic virotherapy enables checkpoint blockade. Nat Rev Drug Discovery. 2018;17:96.
52. Gebremeskel S, Nelson A, Walker B, et al. Natural killer T cell immunotherapy combined with oncolytic vesicular stomatitis virus or reovirus treatments differentially increases survival in mouse models of ovarian and breast cancer metastasis. J Immunother Cancer. 2021;9:e002096.
53. Krabbe T, Marek J, Groll T, et al. Adoptive T cell therapy is complemented by oncolytic virotherapy with fusogenic VSV-NDV in combination treatment of murine melanoma. Cancers. 2021;13:1044.
54. Fang L, Tian W, Zhang C, et al. Oncolytic adenovirus-mediated expression of CCL5 and IL12 facilitates CA9-targeting CAR-T therapy against renal cell carcinoma. Pharmacol Res. 2023;189:106701.
55. Wang S, Li Y, Xu C, Dong J, Wei J. An oncolytic vaccinia virus encoding hyaluronidase reshapes the extracellular matrix to enhance cancer chemotherapy and immunotherapy. J Immunother Cancer. 2024;12:e008431.
56. Boulton S, Singh S, Organ B, et al. Oncolytic vaccinia virus encoding constitutively active EPAC remodels the tumor microenvironment to enhance therapeutic efficacy with chemotherapy and surgery. J Immunother Cancer. 2026;14:e013832.
57. Peng Z, Kalim M, Lu Y. Improving systemic delivery of oncolytic virus by cellular carriers. Cancer Biol Med. 2025;21:1104-19.
58. Yoon A, Hong J, Li Y, et al. Mesenchymal stem cell-mediated delivery of an oncolytic adenovirus enhances antitumor efficacy in hepatocellular carcinoma. Cancer Res. 2019;79:4503-14.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.